
INTRODUCTION
Sparring-Taekwondo (S-TKD) is a full-body contact sport that has been an official sport of the summer Olympic games since 2000 when it gained the additional name of Olympic-style taekwondo. Attacks and counter-attacks for all types of taekwondo permit the legal scoring of kicking techniques directed toward the head/face/neck (i.e., head kicks) and torso, though punching the head region is illegal. Given the kicks used in S-TKD, there is a high risk for brain and musculoskeletal injury in competition and training sessions. A number of studies have reported injury rates in S-TKD competitions [1–9]. In one report, 1,466 injuries occurred in 283 athletes during training, with an average of 5 injuries per athlete annually [10]. A meta-analysis found an injury rate of 79 per 1,000 athlete-exposures (A-E) in taekwondo competitions [6]. Similarly, a recent study of an S-TKD team from Korea has reported injury incidence rates in training sessions and competition of 5 and 25 per 1,000 A-E, respectively [9].
In addition to the musculoskeletal injuries in S-TKD, there is a high risk of concussion, ranging was from 0.0 to 50.2 per 1,000 A-E [11] which is anticipated since a direct kick to the opponent’ s head region is legal and promoted by the competition rule. Additionally, changes made by the sport’ s governing bodies (i.e., World Taekwondo (WT) and Korea Taekwondo Association (KTA) include a recent competition rule (i.e., 2018) where a valid head kick (HK) will be awarded from a minimum of 3 points to a maximum of 5 points (i.e., given higher points). As a result, the head zone has become a major scoring area since 2009. In 2019, the protective scoring system (PSS) was adopted in the competition taekwondo.
Changes to the scoring system for the HK have raised concerns regarding the increasing frequency of HKs and concussions in S-TKD [12–14]. Several epidemiological and biomechanical studies on head impact have been conducted over the last 10 years. Video analyses have con-firmed that the frequency of HKs has increased up to 40% when compared with a study done in 2002 (i.e., when all types of valid HK received 1 point) among youth and elite S-TKD athletes [12–16]. Although there are insufficient studies, follow-up studies revealed that the incidence rates of HKs and concussions seem increased (0.1%) among female high school athletes with no change in rates for male middle school athletes [15,17]. One biomechanical study measured the head impact frequency and magnitude over 6 TKD sparring training sessions involving 8 high school athletes [18]. The results showed that there was a total of 689 head impacts (24 impacts per 100 minutes), of which 97% were low or medium (range 10-69 g) and 3% were high (>69 g).
Since 2002 studies of S-TKD related concussions have been conducted exclusively with youth athletes. Studying S-TKD related head injuries in adults is important given the age groups of Olympic S-TKD athletes and professional S-TKD athletes yet studies for this group are limited. More-over, there is a high possibility of underestimating the incidence rate of concussions reported in the literature due to issues such as recall and selection bias. Sports-related concussion is not only an issue in S-TKD but also in other contact sports due to its short-term and long-term sequelae such as physical performance and neuropsychological problems or chronic traumatic encephalopathy (CTE) [19,20]. Therefore, the purposes of the current study are to estimate incidence rates of HKs and concussions with post-match interviews and to find possible risk factors associated with increased concussion rates among college S-TKD athletes in South Korea.
METHODS
1. Study participants and operational definitions of HK and concussion
A total of 327 college-athletes (female, 119; males, 208) competed in a sparring-taekwondo (S-TKD) tournament held in Kyungnam province, South Korea in July of 2019, completing 311 matches over three days (Table 1). The athletes’ average age was 20.2 years (fehttps://pbs.twimg. com/media/FPrXgzlakAAvChQ?format=png&name=largemale, 22.2, SD±1.8; male, 20.2, SD±1.3). Based on our HK criteria below, we have identified 167 cases of head kicks during a single TKD competition. Of these 167 cases, 109 were interviewed immediately after the conclusion of the match. The remaining 58 athletes declined to be interviewed, and only data from athletes who completed the direct interview were used in the analysis. All athletes were at an advanced level with an average of 8.6 years (SD±2.7) of competition experience.
Table 1.
Number of tournament participants and matches by weight division
We have adapted the same definitions of valid HK and concussion as previous studies [15–17]. The valid HK must be awarded 3-points or more during a match. We defined the definition of a concussion that was considered to have occurred if an athlete who was hit with a valid HK during the match showed common signs and symptoms of physio-logical brain dysfunction including feeling dizzy, stunned, dazed, and/or disoriented. Also, we have included any period of loss of consciousness, memory problems, or neurological issues at the time of the HK.
2. Data collection
Fig. 1 shows our research procedures for data collection. In order to identify HK and concussion cases, observers watched every match and recorded the occurrence of valid HKs at ringside. When noted the valid HK, they recorded the color of the chest protector (red or blue) and match in which the HK occurred, and then reported the case to the athletic trainer or project staff. After the match is over, the athlete who received the HK was asked to go to the interview site, where project staff collected the data. All interviews were conducted at the tournament site by an athletic trainer for 10 to 15 minutes. A simple, structured interview helped by a check-off form (Yes or No) developed by Koh [15–17] was used to collect necessary information on concussion cases. The structured interview case form (Table 2) included 1) demographic information of the athlete; 2) information of HK and concussion, experience of a concussion, post-concussion symptom, past 6-month history of HK and concussion; 3) HK and concussion-related situational information.
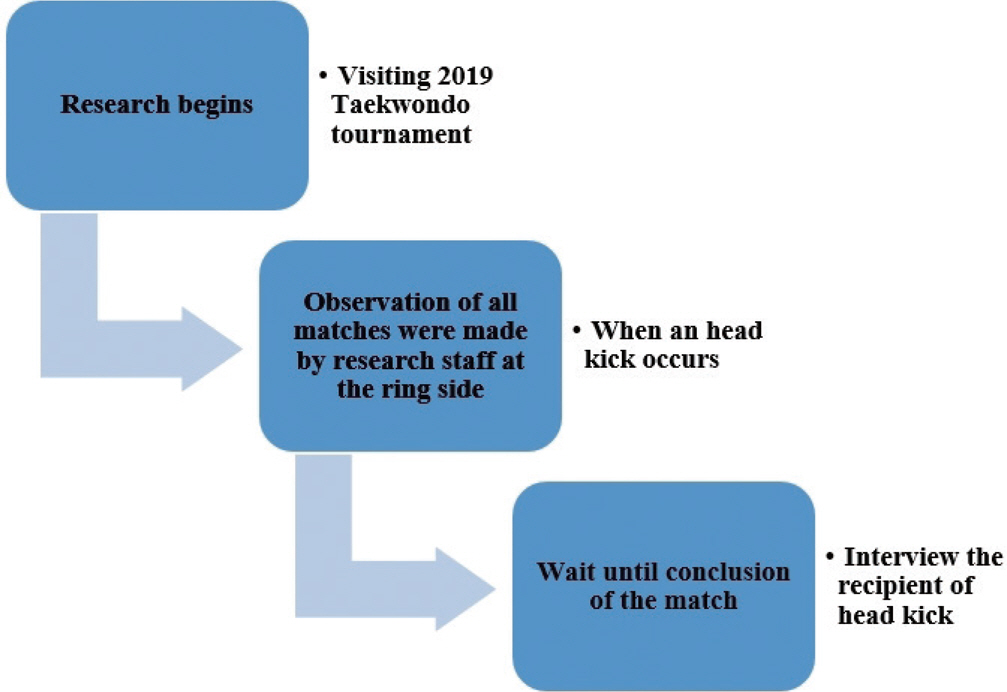
Table 2.
Example of a structured interview case form
All interviewees provided a written informed consent form in compli-ance with the Electronic Institutional Research Board in South Korea in 2019 (e-IRB NO. P01-201906-21-002).
3. Statistical analysis
For estimation of the incidence rates of HKs and concussions, we adapted a formula used in prior incidence studies [4,15-17,21] (# HKs or concussions ÷A-E×1,000=# HKs or concussions per 1,000). The S-TKD match includes two athletes regardless of the individual or group (i.e., 311 matches×2 athletes=622/1,000 athlete-exposure, A-E). One A-E indicates one fighter being exposed to the risk of sustaining an injury [22]. The tournament was a single elimination competition with three rounds, lasting 1.5 (the qualifying match) or 2 minutes (semi-finals and final) per round. To find any association between the dependent and independent variables, a χ-2 test and independent t-test were performed. Furthermore, to determine predictors of the concussions, a binary logistic regression analysis was performed. The alpha level was set at p <.05 and SPSS 26.0 software was used for statistical analysis.
RESULTS
1. Incidence rates for HK and concussion
Table 3 reports the overall injury exposure data. The total incidence rate was 175 HKs per 1,000 A-E (95% CI, 125.2-225.2). Fifty (45.9%) out of 109 athletes received a single HK and the remaining 59 athletes (54%) received two to ten HKs in one match (Table 4). Overall, 256 HKs occurred for the 109 athletes in the study. Table 4 reports the frequency of overall HK occurrence by gender. Female athletes received a higher frequency of HKs than their male counterparts during the tournament (202 vs. 155 HKs per 1,000 A-E, respectively) (Table 3). The average frequency of HKs received per match for females was 2.8 (SD=2.3) and for males was 2.1 (SD=1.3) (Table 4). An independent t-test showed that the difference between male and female athletes was statistically significant (t=-2.053, df=107, p =.04).
Table 3.
Exposure data, incidence of HKs resulting in concussions during the 2019 S-TKD tournament
Table 4.
Overall frequency of HKs by gender
Of the 109 athletes with HKs, 22 experienced a concussion. The total incidence rate of concussion was 35 per 1,000 A-E (95% CI, 1.11-59.7). In particular, female athletes experienced higher concussions rates than male athletes (45 vs. 30 concussions per 1,000 A-E, respectively) (Table 3). Only 27% (6 athletes; 4 males and 2 females) suffered from post-concussion symptoms when interviewed at the conclusion of the match. Symp-toms reported by athletes with a concussion included headache and tiredness (2), dizziness (1), headache (1), balance issue (1), and pressure on the head or neck (1). However, we did not detect amnesia (i.e., asking about the match-related questions) or loss of consciousness.
2. Previous history of HK and concussion
The point prevalence rate of an HK for the last 6-month was extreme-ly high (93.6%, 102 out of 109 athletes). Of these, 50 athletes (45.9%) received an HK at least 5 times. The remaining 59 participants (45.9%) received an HK more than 5 times. In addition, the point prevalence rate of concussion for the previous 6-month period was 15.6% (17 competitors). However, the period prevalence rate of concussion for the entire TKD athlete’ s career was 58.7% (64 competitors: male=38; female=26). Among those with concussions, three cases of loss of consciousness were reported.
3. Frequency of HKs and concussions by weight category
Table 5 shows the overall frequency of HKs and concussions by weight division. Overall, the highest frequency of HKs occurred in the light (19.3%) and fly (18.3%) categories. After adjusting by the actual number of fighters in each weight category, the flyweight division showed the highest frequency of HKs (44%, 20 HKs out of 20 fighters). However, the highest frequency of concussions occurred in the fin weight division (22.7%). The welter and heavyweight divisions recorded the lowest frequency of concussions (4.5% each).
Table 5.
Overall frequency of HKs and concussions by weight category and gender
4. Other possible factors related to concussion
Eighty-one athletes (74.3%) recalled the moment received the HK. Of these athletes, only nine (11.1%) experienced a concussion. Of the remaining 28 athletes that did not recognize receiving the HK, 13 (46.4%) experienced a concussion. We found that there was a significant difference between the concussion rate with or without recognition of the HK (χ2 =16.110, df=1, p =.0001).
Fifty-two players (47.7%) reported using a defensive maneuver when they were attacked by opponents. Among these players, only four athletes (7.7%) experienced a concussion. Conversely, of the remaining 57 players (52.3%) who did not use a blocking maneuver, 18 (31.6%) experienced a concussion. Surprisingly, 64 competitors (58.7%) out of 109 reported that they did not train blocking skills against an HK during reg-ular training sessions.
Table 6 presents the types of kicking techniques that resulted in an HK and concussion. The most frequent skill that resulted in an HK and concussion was the axe kick. The technique with the lowest frequency but the greatest likelihood of a concussion was the 360-spinning kick.
Table 6.
Types of kicking techniques that resulted in a head kick and concussion
We performed a logistic analysis with concussion as the dependent variable, and the other six variables as predictor variables (Table 7). Overall, 109 cases were analyzed and the full model significantly predicted concussion status (omnibus χ2 =28.69, df=6, p =.0001). The model accounted for between 23.1% and 36.5% of the variance in concussion status, with 94.3% of the non-concussed competitors successfully predicted. However, only 45.5% of predictions for the concussed group were accurate. Overall 84.4% of predictors were accurate. Table 7 indicates that only recognition of the HK at the time of receiving it and the use of blocking maneuvers at the time of receiving an HK reliably predicted a concussion. Competitors who did not recognize an HK at the time of receiving it were more likely to experience a concussion (OR, 5.91; 95% CI, 1.65-21.10, p <.05). Additionally, competitors who did not use blocking maneuvers were more likely to experience a concussion (OR, 5.96; 95% CI, 1.61-21.98, p <.05).
Table 7.
Final binominal logistic model
| Variable | B | S.E. | Wald | df | Sig. | Exp (B) | OR (95% CI) |
|---|---|---|---|---|---|---|---|
| Total HKs | -.17 | .20 | .77 | 1 | .37 | .83 | .56-1.24 |
| Gender | -.00 | .65 | .00 | 1 | .99 | .99 | .27-3.60 |
| Recognition of HK | 1.77 | .64 | 7.50 | 1 | .01∗∗ | 5.91 | 1.65-21.10 |
| Past history of concussion | -.56 | .61 | .85 | 1 | .35 | .56 | .17-1.88 |
| Training of Blocking MNVR | .99 | .70 | 2.02 | 1 | .15 | 2.71 | .68-10.71 |
| Usage of Blocking MNVR | 1.78 | .66 | 7.20 | 1 | .01∗∗ | 5.96 | 1.61-21.98 |
| Constant | -3.24 | .94 | 11.75 | 1 | .00 | .03 | - |
DISCUSSION
Because of a lack of studies on the risk of concussion in adult S-TKD athletes, the primary purpose of our study was to measure the true incidence of a concussion directly associated with an HK. We applied an in-terview-based prospective cohort design that allowed us to measure HK and concussion rates with less recall or selection bias. Specifically, S-TKD athletes’ self-reported injuries such as a concussion may be inaccu-rate due to misunderstanding regarding this injury. According to Koh’ s study [17], only 17% of TKD athletes understood they experienced a concussion and less than 10% of athletes experienced a concussion with loss of consciousness. Thus, the significance of this study is to establish an incidence rate of concussion in college competitors and measure the direct HK-related concussion risks among college athletes in S-TKD.
Overall, the incidence rates of HK and concussion were 175 HKs and 35 concussions per 1,000-A-E, respectively. There is clear evidence that the concussion rate has increased when compared to the Pieter and Zemper study [4] (overall, 5.5; male, 7.04; female, 2.42/1,000 A-E when awarding 1-point for an HK). Additionally, when we compared our injury rates to those of high school athletes who competed in 2001 [21], the incidence rate of HK has increased (175 vs. 141 HKs per 1,000 A-E), however, the rate of concussion has remained the same (35 vs. 35.9 concussions per 1,000 A-E). Also, when we compared only females’ incidence rates of HK and concussion to the female high school athletes who competed in 2018 [15] (i.e., HK=3-5 points), the rate of HK is higher (203 vs. 132 HKs per 1,000 A-E), but the rate of concussion is similar (45 vs. 44 concussions per 1,000 A-E). In another comparison to male middle school athletes [17], the present study shows a higher incidence rate of HK among the males (155 vs. 134 per 1,000 A-E). However, our concussion incidence rate is lower than that of middle school athletes (30 vs. 41 per 1,000 A-E). To summarize the differences among studies, there was the age difference, the level of competition, competition rule, and other potential factors such as the headgear sensor adaptation that may influence the present results.
The concussion risk for all HK recipients in the current study was 20.2% (female=22.2%; male=19.3%). When concussion risk is compared to the female high (33.3%) [15] and middle school (35.2%) [16] competitors, our college competitors have a lower rate than the adolescent competitors. Male middle school athletes show a similar trend (31%) [17]. In other words, when interviewing 100 athletes who receive an HK during the tournament, 22-35% of them are likely to occur a concussion.
According to our findings, female athletes recorded higher rates for both HKs and concussions than their counterparts, although the statistical failed to find a significant difference. One study [4] conducted prior to 2002 found results opposite to ours. However, the same results on gender differences of HK and concussion were found in the middle school players [16,17], but not in high school players [21]. A similar trend was observed from the video analysis of the elite level in S-TKD [14]. The high rate of HK-related concussions among females is likely due to females in our study favoring an axe kick which is relatively easy to exe-cute and effective to get high scores from the head kick point. However, a shift in this trend (i.e., an HK by an axe kick) was observed among male athletes in this study. These differences are likely due to changes in the point system for HKs since 2009 [12-14,23]. To verify the issue of gender differences, more research is required.
We did not find an association between a previous history of HKs and concussions and the present incidence rates. The same results were reported from another study with 51 high school female athletes [15]. In contrast, 154 middle school male athletes who had a previous history of concussion had a high incidence rate of concussion [17]. There are several possible reasons for such a discrepancy among studies. First, though there were no differences in study design, the age of research participants differed and the younger age group had a higher risk rate than the older age group [21]. Additionally, the sample size differed between studies, and unlike prior studies, the present study measured both genders. Furthermore, the number of matches per competition is greater in younger groups which results in a longer period of injury exposure which in-creases injury risk as well [21,22].
Two predictors for the increasing risk of concussions were discovered in the current study. Prior studies [15–17] have examined potential risk factors with conflicting results and these inconsistencies among studies remain unclear. Findings from the current study suggest that increased concentration by athletes on their opponent’ s movements during matches may decrease the likelihood of HK and concussion.
The most frequently executed kicking skill for the HKs was an axe kick, yet the most threatening kick that resulted in a concussion was a 360-spinning kick. The axe kick is noted as the most frequent kick in several studies [12-14,17,24]. The 360-spinning kick had a much lower frequency rate but was more likely to result in a concussion. Kicks using spinning techniques such as 360-spinning and roundhouse kicks have similarly been reported as a risk factor for concussions in other studies [15,17,24].
Among 22 athletes with concussions, 27% [6] complained of post-concussion symptoms. In the case of youth S-TKD, male middle school and female high school competitors had a higher rate of 36% [17] and 40% [15], respectively. Headache and dizziness were the most common symptoms. According to our results, the adult group may experience fewer post-concussion symptoms than younger age groups.
As noted previously, a number of athletes declined to participate which may have influenced the incidence rates of both HKs and concussions. Therefore, the reported incidence rates are likely lower than the actual rates in S-TKD tournaments. Also, the incidence rate of concussion was measured by a subjective questionnaire in this study. Additionally, as data collection is based on observation, there is a possibility of some missed cases. Given these limitations, the present injury rates can-not be generalized to all athletic competitions.
CONCLUSION
We found that 22 (20.2%) athletes experienced concussions among 109 HK recipients. The incidence rates of HK and concussion were high in our participants, with female athletes experiencing a higher frequency of HK and concussion than male athletes. However, these incidence rates may have been impacted by a number of athletes who declined to participate and data missed due to observer error. Nonetheless, the cur-
rent study provides further evidence that factors associated with the concussion rate include recognition of receiving an HK at the time of occurrence and the use of blocking maneuvers. Further research is necessary to confirm our observations, to monitor any changes in the concussion risk, to track cumulative negative effects of multiple HKs, and to provide a safer environment for future S-TKD athletes.


