
서 론
급속한 경제발전으로 인구의 고령화 현상은 공중보건문제로 이어지고 있을 뿐만 아니라 고령화 및 노화와 관련된 질병은 사회 전체에 막대한 경제적 부담을 가중화시키고 있다. 특히 인지장애와 치매는 나이와 관련된 흔한 질병의 일종으로 고소득 국가에서 65세 이상 인구의 약 5-10%를 차지하고 있으며, 유병률은 65세 이후 5세마다 두 배로 증가하는 것으로 보고되었다[1]. 이미 국내에서도 노년기 인지장애와 치매가 건강 및 사회복지에 대한 주요 도전과제가 되고 있지만 아직까지 치료에 대한 성공은 제한적인 실정이지만 최근 여러 연구를 통해 다양한 위험인자를 예방하면 위험률을 낮출 수 있는 것으로 나타나 예방 차원에서의 접근이 중요시되고 있다[2]. 따라서 인지장애 및 치매의 잠재적 위험요인, 그중에서도 수정가능한 위험요인을 확인하는 것은 인지저하를 예방하는 최선책이 될 수 있을 것이다[3].
예컨대 나이와 관련된 질병이면서 수정가능한 위험요인 중 하나인 대사증후군(metabolic syndrome)은 심혈관질환의 발병과 직접적인 관련이 있으며, 제2형 당뇨 발병위험을 증가시키는 혈관 및 대사위험 인자의 군집으로 잘 알려져 있다[4,5]. 자세하게 살펴보면 65세 이상 노인에서 혈관위험인자 및 대사증후군의 존재는 관상동맥질환, 뇌졸중 및 사망 위험률이 증가[6,7]할 뿐만 아니라 집행 기능 손상[8], 인지장애[9] 및 치매 발병 위험[10,11]을 높이는 것으로 보고되고 있다. 더욱이 심혈관 및 뇌혈관질환은 당뇨병 또는 비만과 같은 대사질환의 흔한 동반 질환[12]으로 알려졌고, 심혈관질환은 크고 작은 혈관의 병태생리학적 변화를 촉진하여 시간이 지남에 따라 인지장애와 치매로 이어질 수 있다[13]. 최근 다양한 연구에서도 기억[14–16], 집행기능[17,18], 주의력/속도[19,20] 및 전체적인 인지기능[16]은 중년 또는 노년기 대사증후군의 각 구성요소(예, 비만, 당뇨 및 고혈압)와 관련이 높은 것으로 밝혀지고 있다. 반면 간이건강상태 점수를 기준으로 높고 낮은 두 집단을 구분하였을 때, 고혈압, 당뇨병, 심장질환 등의 위험 요인들과의 관련성이 통계적으로 의미가 없고, 나이, 성별, 교육수준을 고려했을 때 대사증후군의 유무가 간이 건강상태 점수에 영향을 주지 않는 것으로 나타나 상반된 결과를 보여주고 있다[21,22].
한편 대사증후군과 함께 노년기 일상생활 및 활동에 영향을 주는 요인으로 체력의 역할 또한 주목을 받고 있다. 연령이 증가할수록 근육의 소실로 인한 근력 및 이동능력이 저하되고 신체활동 감소로 인한 심폐체력이 낮아져 궁극적으로 만성질환 유병률을 높인다[23]. 특히 심폐체력은 대사증후군 위험을 예측하는 주요 요인으로서 낮은 심폐체력 수준과 운동부족은 심혈관질환 위험을 초래할 뿐만 아니라 노년기 인지기능저하와 부적 상관성을 나타내는 것으로 보고되었다[24]. 반면 노년기 심폐체력이 향상되면 인지기능 저하를 예방[25]하는 데 도움이 될 수 있고, 심폐체력이 높은 노인은 일시적 사건에 대한 기억이 젊은 성인보다는 낮지만 심폐체력이 낮은 노인보다는 우월하며[26], 심폐체력이 높은 노인에서 젊은 성인과 동등하게 집행기능을 유지[24]할 수 있는 것으로 나타났다. 장기간의 종단연구에서도 심폐체력수준이 낮은 사람들의 인지기능은 나이가 들어갈수록 현저하게 감소[27,28]하는 것으로 나타나 심혈관 건강의 중요한 영역 중 하나인 심폐체력 또한 중∙노년기 인지기능과 관련이 있을 것으로 판단된다.
이와 같이 대사증후군과 낮은 심폐체력은 인지기능 저하에 대한 수정가능한 위험인자로 잘 알려지면서 노년기 생활습관의 변화를 통해 인지장애 또는 치매의 발병을 늦추거나 예방할 수 있음을 시사하고 있다. 그러나 노인을 대상으로 대사증후군 또는 심폐체력 수준이 인지장애에 미치는 독립적인 역할에 대해 상반된 결과와 함께 위험인자 간의 복합적인 관계를 분석한 연구는 부족한 실정이다.
따라서 본 연구는 노인을 대상으로 객관적이면서 누구나 안전하게 측정할 수 있는 6분 걷기를 활용[29]하여 심폐체력 수준을 확인하고, 노년기 인지장애 노출 위험에 대한 대사증후군과 심폐체력의 독립적 그리고 복합적인 관계를 확인하고자 하였다.
연구 방법
1. 연구대상
본 연구는 횡적연구(cross-sectional study) 설계를 기반으로, 의학적으로 특별한 질환이 없고, 정상적인 일상생활 수행이 가능한 경기도 S 시 지역 경로당 및 편의시설 등에 왕래하고 있는 65세 이상 재가노인을 대상으로 하였다. 실험 시작 전 모든 참여자에게 실험의 목적과 절차에 대해 충분히 설명하고, 자발적으로 동의서에 서명한 후 참여하도록 하였다. 최초 542명을 모집하였으며, 체력측정 또는 혈액검사 미참여자 24명과 개인사정으로 인한 중도 탈락자 9명을 제외하고 총 509명을 대상으로 분석하였다. 이와 같은 모든 절차는 실험 전 연구윤리심의 위원회의 승인을 받은 후 실행하였다(SKKU 2018-06-005-003).
본 연구에 참여자의 일반적 특성은 Table 1과 같다.
Table 1.
Descriptive statistics of study participants
2. 측정변인
1) 신체조성
신장(cm)과 체중(kg)은 자동신장계측기기(DS-102, Jenix, Seoul, Korea)로 측정하였으며, 체지방률과 제지방량은 다주파수 임피던스기기(Inbody 720, Biospace, Korea)를 이용하여 측정하였다. 체질량지수(body mass index, BMI)는 [체중(kg)/신장(m2)] 공식으로 산출하였다.
2) 대사증후군
각 참여자들은 실험 전 최소 10시간 이상 공복 상태를 유지한 후 상완정맥에서 약 4 mL 정도의 혈액을 채취한 후 자동화학분석기 AD-VIA 1650 Chemistry system (Bayer, Tarrytown, NY, USA)을 이용하여 중성지방(mg/dL), 고밀도지단백콜레스테롤(mg/dL) 및 공복 시 혈당(mg/dL)을 분석하였다. 허리둘레(cm)는 늑골 하단부(lower border of rib cage)와 장골능 상부(top of iliac crest) 간 중간부위에서 측정하였으며[30], 2회 측정 후 평균값으로 기록하였다. 이때, 측정 간 오차 범위가 ±0.5 mm 이상일 경우 재 측정하였다. 안정 시 혈압(mmHg)은 실험실 도착 후 10분 이상 안정을 취한 상태에서 자동혈압계(FJ-500R, Jawon Medical Co., Seoul. Korea)로 측정하였고 2회 측정 후 평균값을 기록하였으며, 측정 간의 간격은 2분으로 하였다. 본 연구에서는 NCEP ATP Ⅲ (National Cholesterol Education Program Adults Treatment Panel Ⅲ) [31] 가이드라인을 기준으로 중성지방(TG, ≥150 mg/dL), 고밀도지단백콜레스테롤(HDL-C, 남 <40 mg/dL, 여 <50 mg/dL), 공복 시 혈당(FBG, ≥100 mg/dL 또는 약물복용 중), 허리둘레(남 ≥90 cm 여 ≥85 cm) [32] 그리고 안정 시 혈압(수축기 ≥130 mmHg 또는 이완기 ≥85 mmHg 또는 약물복용 중) 중 3가지 이상 포함될 경우 대사증후군으로 진단하였다.
3) 심폐체력
본 연구에서는 누구나 안전하고 쉽게 참여할 수 있고, 특히 노인을 대상으로 신뢰도와 타당도가 검증된 6분 걷기 검사를 이용하여 심폐체력수준을 추정하였다[29,33]. 참여자들은 6분 동안 50 m 길이의 트랙에서 연속적으로 가능한 빨리, 더 멀리 걷도록 하였으며, 이때 매 분마다 남은 시간을 알리면서 격려를 하였다. 최종적으로 6분이 종료된 시점에 개인이 간 거리(m)를 기록하였다. 측정된 기록을 기준으로 한국스포츠정책과학원에서 개발한 질병예방을 위한 노인기 건강기준 체력 수준 지표[34]를 활용하여 성별과 나이를 고려한 심폐체력수준에 따른 정상그룹(normal CRF group)과 낮은 그룹(low CRF group)으로 구분하였다.
4) 인지기능
인지기능은 Folestein et al. [35]이 개발한 간이정신건강상태 검사를 기초로 한국 노인의 인구학적 그리고 문화적 특성이 반영된 치매 선별용 한국어판 간이정신상태 검사(Korea version of Mini-Mental State Examination for Dementia Screening, MMSE-DS) 도구[36]를 이용하였다. 모든 검사는 외부 노출 없이 1:1 면접방식으로 동일한 검사자가 실시하였다. MMSE-DS는 시간지남력 5문항, 장소지남력 5문항, 기억력 2문항, 주의집중력 1문항, 언어능력 2문항, 실행력 1문항, 시공구성능력 1문항 그리고 판단 및 추상적 사고력 2문항 총 19문항으로 구성되어 있다. 원점수는 0점에서 최고 30점으로, 성별, 연령, 학력수준의 기준에 따른 표준 정상점수를 통해 인지장애 유무를 판정한다. 본 연구에서 활용된 MMSE-DS의 Cronbach’α는 .91로 나타났다.
3. 자료분석
본 연구의 모든 자료는 평균과 표준편차(mean±SD)와 n (%)로 표기하였다. 대사증후군 유무와 심폐체력수준에 따른 측정 변인 간의 비교를 위해 연속변수는 독립 t-test와 비연속변수는 카이제곱 검증(chi-square test)을 이용하였으며, 대사증후군위험인자 개수에 따라 간이정신건강상태 점수 비교는 Kruskal-Wallis test를 통해 선 경향(linear trends) 유무를 확인하였다. 또한 인지장애노출 위험에 대한 대사증후군과 심폐체력수준에 따른 복합적 효과를 검증하기 위해 다항로지스틱 회귀분석(multinomial logistic regression)을 이용하여 승산비(odds ratio, OR)와 95% 신뢰구간(confidence interval, CI)을 산출하였다. 모든 자료의 통계분석은 SPSS-PC (version 20.0)를 이용하였으며, 가설검정을 위한 유의수준은 α=.05로 설정하였다.
연구결과
1. 대사증후군 유무에 따른 신체적 특성과 간이정신건강상태 점수 비교
Table 2는 대사증후군 유무에 따른 신체적 특성과 간이정신건강상태 점수를 비교한 것이다. 대사증후군에 노출된 노인이 대사증후군이 아닌 노인보다 나이(p <.001)가 많았고, 체질량지수(p <.001)와 복용 약 개수(p <.001)가 높았으며, 6분 걷기(p =.005) 그리고 간이정신건강상태 점수(p <.001)가 낮은 것으로 나타났다. 게다가 Fig. 1에 제시한 바와 같이 대사증후군 위험인자 개수가 증가함에 따라 간이정신건강상태 점수(F(3,1) =91.464, p =.012)가 통계적으로 유의한 선 경향성이 있는 것으로 나타났다. 이는 대사증후군 위험인자가 1개 증가하면 증가할수록 간이정신건강상태 점수가 감소한다는 사실을 의미하는 것으로 해석된다.
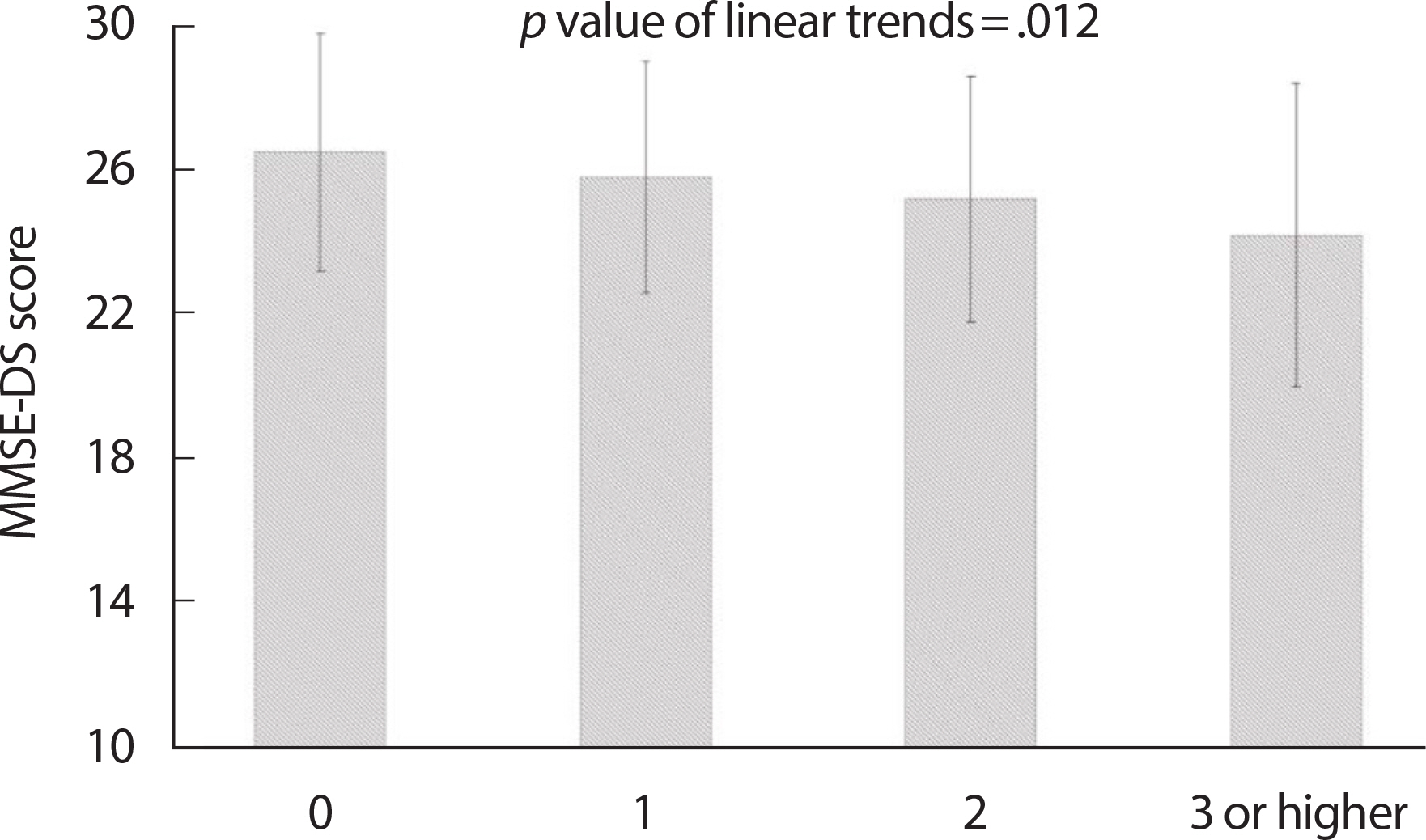
Table 2.
Difference of physical characteristics and MMSE-DS score according to metabolic syndrome status
2. 심폐체력 수준에 따른 신체적 특성과 간이정신건강상태 점수 비교
Table 3은 심폐체력 수준에 따른 신체적 특성과 간이정신건강상태 점수를 비교한 것이다. 성별 및 연령을 보정한 심폐체력수준이 낮은 노인이 정상수준인 노인보다 나이(p <.001)가 많았고 체질량지수(p <.001)와 허리둘레(p <.001)가 높았으며, 간이정신건강상태 점수가 낮은(p <.001) 것으로 나타났다. 또한 심폐체력수준이 낮은 노인이 정상수준 노인보다 대사증후군 요인 개수(p =.004)가 더 많은 것으로 나타났다.
Table 3.
Difference of lifestyle risk factors and MMSE-DS score according to cardiorespiratory fitness levels
BMI, body mass index; WC, waist circumference; SBP, systolic blood pressure; DBP, diastolic blood pressure; FBG, fasting blood glucose; TG, triglyceride; HDL-C, high density lipoprotein cholesterol; MetS criteria, metabolic syndrome criteria; MMSE-DS, mini-mental state examination of dementia screening.
3. 대사증후군 유무와 심폐체력 수준에 따른 인지장애 노출 위험 수준 비교
Fig. 2는 대사증후군유무와 심폐체력 수준에 따른 인지장애에 노출될 위험 수준을 비교한 것이다. 나이, 교육수준, 체질량지수, 허리둘레, 약 복용, 음주, 흡연 그리고 신체활동을 포함한 교란 변인을 통계적으로 보정한 결과, 대사증후군이 아니면서 정상적인 심폐체력 수준을 가진 노인(no MetS and normal CRF, OR=1)에 비해 대사증후군이면서 정상적인 심폐체력 수준을 가진 노인(MetS and normal CRF, OR= 1.747, 95%CI=1.044-2.923, p =.043), 대사증후군이 아니면서 낮은 심폐체력 수준을 가진 노인(no MetS and low CRF, OR=2.246, 95CI=1.146-4.402, p =.018), 그리고 대사증후군이면서 낮은 심폐체력을 가진 노인(MetS and low CRF, OR=3.066, 95%CI=1.711-5.492, p =.001)이 인지장애에 노출될 위험이 상대적으로 더 높은 것으로 나타났다.
Fig. 2.
Fig. 2.Association combined of metabolic syndrome and cardiorespiratory fitness levels on cognitive impairment. Odds ratio (OR) and 95% confidence interval (CI) for cognitive impairment according to metabolic syndrome (MetS) - and cardiorespiratory fitness (CRF) levels-based subgroups. ORs were adjusted for covariates, including age, education, body mass index, waist circumference, medications, alcohol intake, smoking, physical activity.

논 의
본 연구는 65세 이상 노인을 대상으로 대사증후군 및 심폐체력 수준과 인지장애 간의 관계성 분석을 통해 대사증후군과 심폐체력이 인지장애 노출 위험인자로써 갖는 독립적 그리고 복합적 의미를 밝히고자 하였다. 그 결과, 정상적인 노인에 비해 대사증후군 노인은 심폐체력수준이 낮았고, 낮은 심폐체력 수준을 가진 노인은 대사증후군 위험인자 개수가 더 많은 것으로 나타났다. 또한 대사증후군 또는 낮은 심폐체력수준의 노인은 정상노인에 비해 인지장애 노출 위험이 높게 나타나 2가지 독립적인 예측인자인 대사증후군과 심폐체력 수준이 인지장애 위험에 대한 뚜렷한 차이를 보였으며, 특히 대사증후군이면서 낮은 심폐체력을 가진 노인에서 인지장애 노출 위험률이 가장 높은 것으로 나타났다. 이러한 결과는 대사증후군과 심폐체력이 인지장애 노출 위험에 있어서 독립적 그리고 복합적으로 관계가 있다는 것을 의미한다.
자세히 살펴보면 좌식행동 습관, 중 ∙고강도 신체활동 및 심폐체력은 대사위험의 예측인자이며[37,38], 그중에서도 심폐체력은 고령자의 모든 원인으로 인한 사망률 및 유동성을 가장 잘 예측하는 인자 중 하나로 알려지면서 노년기 심폐체력의 중요성이 강조되었다[39,40]. 본 연구 결과와 유사하게 노인 또는 성인을 대상으로 한 국내외 선행연구에서도 심폐체력과 대사증후군 사이의 역 상관관계가 있다는 것이 밝혀졌다. 예로, 심폐체력 및 근력 수준은 노년기 대사증후군 유병률과 반비례하고 독립적인 관계가 있고[41], BMI와 낮은 심폐체력은 대사증후군의 높은 유병률[42]과 관련이 있는 것으로 나타났으며, 특히 당뇨병이 있는 노인에서 6개월간 유산소 운동 중재 후 심폐체력과 인슐린 감수성의 개선을 확인하면서 혈당 조절과 적절한 생활습관의 중요성이 보고되었다[43]. 게다가 Kim et al. [44]은 과체중 및 비만 성인을 대상으로 내장지방과 심폐체력, 대사증후군과의 관계를 분석한 결과, 높은 내장지방과 낮은 심폐체력 수준은 대사증후군 유병률을 더욱 높일 수 있다는 것을 발견함과 동시에 대사증후군과 내장지방 사이의 관계를 결정하는 수정인자로서 심폐체력의 역할을 강조한바 있다. 이는 복부비만 또는 내장지방은 중성지방의 증가와 HDL-C 감소 그리고 인슐린 저항성과 밀접하게 관련되어 있고[45], 심폐체력은 과체중/비만[46], 정상인[47] 모두에서 인슐린 감수성 및 인슐린 작용과 긍정적인 관련이 있으며, 항염증을 강화하면서 염증유발을 억제함으로써 대사증후군 노출에 대한 보호 역할[48]을 하는 것으로 판단된다.
한편, 본 연구에서 대사증후군과 심폐체력, 그리고 인지장애와의 관계를 분석한 결과 노년기 인지장애에 대한 대사증후군과 심폐체력의 독립적 그리고 복합적인 관련성을 확인하였다. 이미 다양한 선행 연구를 통해 인지기능에 영향을 미치는 여러 요인 중 대사증후군 또한 중요한 위험 인자인 것이 밝혀졌고[49,50], 대규모 장기 추적연구를 통해서도 대사증후군이 치매 진행을 가속화시킬 수 있다는 가설이 제기되면서 알츠하이머성(Alzheimer's disease) 치매 또는 혈관성 치매의 위험인자로 밝혀졌다[51,52]. 최근 연구에서도 대사증후군은 주의력/지각속도, 실행 기능 및 언어 유창성 영역에서 낮은 인지능력과 관련이 있고[53], 연령, 성별, 흡연 및 심혈관질환과 상관없이 HDL-C이 낮고 TG가 높으면 인지장애가 발생할 가능성이 높아지는 것으로 보고되었다[54]. 흥미롭게도 중년기의 비만[55], 이상지질혈증[56] 및 고혈압[57]은 신경병변 유형의 알츠하이머성 질환을 포함한 후기 인지장애[58,59]와 밀접한 연관성이 있다는 사실이 알려지면서 중년 또는 노년기 대사증후군의 구성요소가 인지장애 및 치매위험 증가에 영향을 미치는 것으로 나타났다. 이것은 아마도 혈관 보호 및 항 염증 역할을 하는 HDL-C 기능과 인슐린 수용체의 민감성 변화를 통해 혈관의 병변으로 인한 신경전달능력 저하로 이어져 처리속도를 포함한 다양한 인지기능 장애를 유발하는 것으로 판단된다. 실제로 Yau et al. [60]은 대사증후군으로 인해 발생한 당대사장애가 중추신경계의 초기 생리적 단계에 영향을 미쳐 궁극적으로 뇌의 구조적 변화의 원인이 될 수 있다고 제안한 바 있다.
더욱이 노년기 인지기능과 대사증후군과의 관계뿐 아니라 심폐체력과의 연관성 또한 연구가 활발하게 지속되고 있다. 오래전 Brown et al. [61]은 높은 심폐체력 수준과 혈관 및 혈액순환 기능과의 강한 연관성을 밝히면서 인지기능에 대한 심폐체력과 뇌 혈류량의 관계를 강조하였으며, Schultz et al. [24]은 노인 및 중년 성인의 최고산소섭취량(VO2 peak)과 아밀로이드 베타(Amyloid-beta, Aβ), 언어 학습 및 기억력 간의 높은 관련성 있고, Pentikainen et al. [62]은 심폐체력이 인지기능에 전반적으로 영향을 미치기보다는 실행 및 추론과 같은 전두엽 영역에 더 의존하는 인지능력의 선택적 향상과 관련이 있는 것으로 보고하였다. 또한 Ericsson et al. [63]은 중년 및 노년층을 대상으로 12개월 동안의 운동 참여가 기억을 담당하는 해마의 질량을 유의하게 증가시켰고, 특히 Netz et al. [25]은 나이가 들어서도 심폐체력이 향상되면 인지기능저하를 예방하는 데 도움이 될 수 있으며 뿐만 아니라 Hayes et al. [26]은 심폐체력이 높은 노인은 젊은 성인과 동등한 집행기능(executive functions)을 유지할 수 있다고 보고하였다. 반면 최근 많은 중재연구를 통해서 운동에 참여하는 것은 인지기능 향상에 긍정적인 영향을 미치는 것으로 밝혀졌다[64,65]. 하지만 España-IrIa et al. [64]은 뇌의 구조와 기능의 변이가 인지기능저하의 행동 증상이 시작되기 전 수년에 걸쳐 발생하고, 더 좋은 인지기능이 더 높은 수준의 체력으로 이어질 수 있다는 잠재적 근거를 제안한 바 있으며, Sabia et al. [67]의 대규모 종단 연구에서도 중등도 신체활동의 참여는 치매 진단을 받기 약 8-12년 전부터 감소하기 시작했으며 최종적으로 치매진단을 받지 않은 사람들의 경우 총 신체활동이 노년기에 걸쳐 계속 증가하는 것으로 밝혀졌다. 이러한 결과는 나이가 들어감에 따라 뇌 건강 및 인지기능을 최적화하기 위해 심폐체력을 유지하는 것이 중요해지는 중년 초기부터 후반까지의 기간이 존재한다는 것으로 판단된다.
이와 같이 심폐체력과 인지기능의 관계는 양방향일 수 있고, 이러한 방향성을 확인하는 것은 제한적이다. 더욱이 심폐체력의 감소와 심혈관 및 대사위험 인자의 증가는 나이가 들면서 발생하지만 이것이 어느 정도 내재적 노화의 결과인지 또는 노화와 생활습관 요인의 상호작용의 결과인지는 아직 불분명한 상태이다.
따라서 대사증후군 또는 낮은 심폐체력을 가진 개인을 조기에 식별하고 예방하는 것은 노년기 인지기능 저하 위험을 줄이는 데 중요한 역할을 할 수 있을 것이며, 특히 심폐체력 증진 및 대사증후군 위험 감소를 위한 규칙적인 신체활동에 참여하는 것이 중요할 것으로 판단된다.
결 론
본 연구는 65세 이상 노인을 대상으로 대사증후군 및 심폐체력 수준과 인지장애 간의 관계성 분석을 통해 대사증후군과 심폐체력이 인지장애 노출 위험인자로써 독립적 그리고 복합적으로 미치는 영향을 분석하였다. 그 결과, 노년기 대사증후군을 가진 노인 그리고 낮은 심폐체력을 가진 노인에서 각각 간이정신건강상태 점수가 낮은 것으로 나타났다. 특히 대사증후군이면서 낮은 심폐체력을 가진 노인에서 간이정신건강상태 점수가 가장 낮은 것으로 확인되었다.
따라서 본 연구결과를 종합해 볼 때, 노년기 대사증후군 또는 낮은 심폐체력을 확인하는 것은 인지장애 위험을 조기에 식별하고 관리하는데 있어서 우선적으로 시행되어야 할 것이고, 더불어 신체활동을 포함한 생활습관 수정은 인지장애 발병 위험을 줄이기 위한 치료 전략이 될 수 있을 것으로 판단된다.


