
INTRODUCTION
Gynecologic cancers, including the cervix, endometrium, fallopian tubes, ovaries, uterus, and vagina refers to the uncontrolled growth and spread of abnormal cells originating in the female reproductive tract. This cancer is one of top ten leading cancer types regarding estimated new cancer cases by sex. Approximately 98,280 (12.1%) new cases were diagnosed as genital cancer in the United States [1] and 6,025 (5.9%) cases were diagnosed as cervical, ovarian and endometrial cancers in South Korea [2] in 2015. According to the International Federation of Gynecology and Obstetrics (FIGO) staging systems, gynecologic cancer consists of four stages and subdivisions. The 5-year survival rate for gynecologic cancers by stage is detected as 89%, 66%, 34%, and 18% respectively for Stage I, II, III, and IV [3]. The proportion of cancer survivors has been increased due to the advances of modern medicine. According to study the survival rate of gynecologic cancer patients will rise by 118% from 2016 to 2026 [4]. However, gynecologic cancer treatment including surgery, chemotherapy, and radiotherapy can give severe damage to pelvic floor muscles (PFM) that could make adverse effects such as pelvic floor dysfunction (PFD), lower extremity lymphedema, emotional concern and fatigue [5,6]. As a result, it became important to identify the adverse effects that frequently occur in the patient with gynecologic cancer and to find out an effective way to alleviate them.
PFM are located inside the pelvis consist of twelve striated muscles with three-layer muscular plate supporting pelvic organs such as urethra, vagina and rectum. During the cancer treatments, atrophy and length shortening may occur in PFM which may result PFD [7]. The symptoms of PFD are known as urinary incontinence (UI) and urgency, hematuria, vaginal and rectal bleeding, dysuria, vaginal dryness and stenosis, dyspareunia and decreased sexual interest [8-11]. Among them, UI is closely related to PFD that can be recovered through pelvic floor muscle training (PFMT). According to the previous studies the PFMT program was effective treatment on women with stress, urge, and mixed urinary incontinence [12]. PFM plays an important role in preventing UI by tightening the urethra. Thus, PFMT may increase the strength of these muscles [13]. The PFMT introduced by Kegel in 1952 for the first time and over time different training protocols have been adopted to improve PFM function [14]. PFMT recognized as the mostly common nonsurgical treatment for UI, which is a physical training program consists of repetitive contraction of the PFM to improve strength and efficacy [15]. In overall, PFMT protocol contains fast contractions of PFM with a 3-second hold to improve strength and few repetitions of longer contractions up to 10 seconds holding with a goal of enhancement in muscle endurance. Though set and repetition of performance are various in studies, more than 3 sets of performance per day and 10 repetitions are often reported in the previous studies [16]. The PFMT program generally consists of contraction of the adductor muscles, sphincter tightening, and pelvic lifting. PFMT is basically doing by weight bearing, but also the resistance band or ball can be used to increase the exercise intensity. One study reported 84% of patients were cured from UI by doing PFMT [14,17]. Although the effects of the training are well studied in women [18], men with prostate cancer patients [19-21], pregnant and postpartum women [22], yet, it has not been fully studied on gynecologic cancer patients. Therefore, the aim of this study is to identify UI type and incidence rate in the gynecologic cancer patient. Also, review the previous intervention studies that had a kinematics approach to improve UI symptom in non-cancer patients as studies are insufficient for gynecologic cancer. Finally, we investigate some of PFMT studies in the patient with gynecologic cancer to discuss the applicability of PFMT to reduce UI based on positive evidences.
METHODS
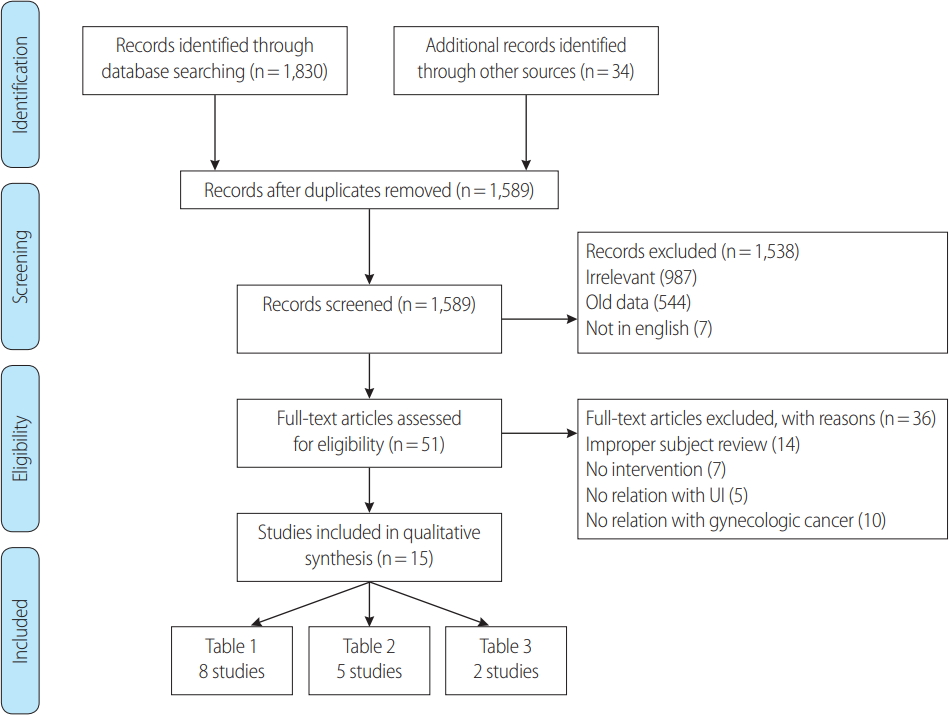
In this review article, we investigated studies through searching in the PubMed, Google Scholar, SCOPUS, EBSCOHost, ScienceDirect, Cochrane Library and EMBASE databases. We limited our search based on language (i.e., English), date of publication (i.e., since 2008 till 2018, last 10 years), the type of article (i.e., journal article), text availability (i.e., full text available) and focusing on previous literature which had the terms of “pelvic floor muscle training”, “urinary incontinence” and “gynecologic cancer” in title or abstract. In primary search, those studies which reported the UI prevalence in gynecologic cancers such as Cervical, Ovarian, Uterine, Vaginal and Vulvar cancers were selected. The secondary selection of articles was limited to those studies which reported UI changes following PFMT either in gynecologic cancer patients or non-cancer patients. Articles were reviewed by two authors independently. At the end, after removing duplicates and non-relevant articles, a total of 15 articles met the criteria; 8 studies (n=2,799) for investigating the UI prevalence among gynecologic cancer patients; 5 studies (n= 444) in non-gynecologic cancer patients and 2 studies (n= 64) in gynecologic cancer patients which reported UI outcome after PFMT were selected for ongoing review (Fig. 1). In addition, we used PEDro scale to measure methodological quality of clinical trials.
THE PREVALENCE OF URINARY INCONTINENCE
Eight studies met the criteria for our studies which reported outcomes in association to UI including SUI and UUI. Most studies were designed in cohort and cross-sectional. Except for the two studies [23,24] which reported the prevalence of UI before any treatment and surgery, the rest of studies reported outcomes after or during treatment (e.g., surgery, chemotherapy, radiation). The prevalence of UI in 2,423 survivors of major gynecologic cancers mostly cervical, endometrial and ovarian cancer before and after treatment is summarized in Table 1.
Of eight studies investigating UI, six studies used validated questionnaires. Bretschneider et al. [23] used International Consultation on Incontinence Questionnaire Female Lower Urinary Tract Symptoms Module (ICIQ-FLUTS) while Donovan et al. [25] used ICIQ-FLUTS along with Memorial Symptom Assessment Scale (MSAS). Rutledge et al. [26] and Skjeldestad et al. [27] used Sandvik Incontinence Severity Index. Hazewinkel et al. [10] used a set of a set of validated pelvic-floor-related quality of life questionnaires included the Uro-genital Distress Inventory (UDI) and the Defecatory Distress Inventory (DDI). Segal et al. [28] used Questionnaire for Urinary Incontinence Diagnosis (QUID) and Incontinence Severity Index questionnaire (ISI). Among gynecologic cancer patients SUI and UUI rates ranged from 30.8% [24] to 59.5% [23] and 13.9% [24] to 33.9% [23] before treatment, respectively. Among the gynecologic survivals, range of SUI reported from 24.3% [27] to 76% [25] while UUI reported from 9.3% [27] to 75% [25]. Regarding to type of treatment, Segal et al. investigated the effect of radiation therapy as a risk factor of pelvic floor function and reported 21.0% SUI and 13% UUI prevalent among “radiation therapy” group while 24.1% SUI and 26.4% UUI reported in “No radiation” group which concluded there is no association between radiation and urinary incontinence (p>.05); whereas age (aOR=1.06, 95% CI 1.02-1.10) and BMI (aOR=1.07, 95% CI 1.02-1.11) significantly were observed as risk factors for UI. However, Hazewinkel et al. reported the result for each treatment group and conclude that patients who treated with radiotherapy as primary treatment more suffered of adverse effects on pelvic floor function rather than surgery with adjuvant radiotherapy or radical hysterectomy (57% UUI [OR=3.7, 95% CI 1.5-8.9] and 53% SUI [OR=1.0, 95% CI 0.5-2.4]). In Buchsbaum et al. [29] study that the prevalence of UI was similar among benign and malignant patients.
PELVIC FLOOR MUSCLE TRAINING FOR THE NON-CANCER PATIENT WITH URINARY INCONTINENCE
Five studies were selected to define the effect of PFMT in UI patients with non-gynecologic cancer. Castro et al. [30] reported that the effectiveness of PFMT was similar with other treatment such as electrical stimulation and vaginal cones based on objective and subjective evaluations. The treatments which include PFMT were far superior to no-treatment in women with SUI. However, high costs and the necessity of regular management were mentioned as the major concerns in various types of UI treatment, except for PFMT. In other study, symptoms of UI was significantly decreased in both SUI and UUI groups where home-based PFMT was conducted with no supervision [31]. Thus, PFMT might be a good alternative choice on UI patients. Besides, as the risk of developing gynecologic cancer is getting higher with ageing, PFqMT may be an appropriate exercise program for the elderly who are not free to go outsides, if adequate training is provided [32,33]. Two studies suggest PFMT can be a good therapeutic option for improving UI in elderly women. According to the results that showed the improvement was more prominent in women with SUI, it is concluded that PFMT is necessary especially for gynecologic cancer patients who are more suffering from SUI than UUI as shown in the Table 2. However, qualitative evaluation of UI symptoms by questionnaire might be considered as a limitation of this study. Tosun et al. assessed PFM strength by using vaginal biofeedback and transabdominal ultrasonography and reported significant improvement in muscle strength after training and the pad test for UI showed significantly decreased in PFMT group [34]. Efforts to use the noninvasive and quantitative method to identify the change in pelvic floor muscle after PFMT seems valuable in this study while quantitative assessment tools are deficient.
PELVIC FLOOR MUSCLE TRAINING FOR THE GYNECOLOGIC CANCER PATIENT WITH URINARY INCONTINENCE
Only two PFMT intervention studies on gynecologic cancer patients were found (Table 3). In the study by Yang et al. [35] patients who had radical hysterectomy and pelvic lymph node dissection were recruited to participate in the pelvic floor rehabilitation program once a week for four weeks. Unlike other studies, this study focused on patients who underwent surgery as a cancer treatment. Additional studies should be continued to identify PFMT effects by differentiation cancer treatment methods such as radiotherapy and chemotherapy. Of many variables, only pelvic floor strength and sexual functioning showed significant improvement. The reason for this result may be influenced by the intervention period which was short to accommodate study feasibility and to verify the effects of exercise. A large scale of intervention with a sufficient study period is necessary. Another pilot study demonstrated PFMT program in combination with behavioral therapy for 12 weeks [36]. Although results did not show the superiority of PFMT on behavioral therapy in the improvement of UI, this study was a rare evidence that PFMT to the gynecologic patient.
RESULT AND DISCUSSION
Through this review, we found that urinary incontinence following gynecologic cancer treatment appeared as a significant adverse effect. Among the types of urinary incontinence, SUI was the most common one, followed by UUI. The studies which were covered in this review were based on a questionnaire. Thus, it is a major limitation of current evidence that makes it impossible to compare the outcomes of research statistically. Moreover, there is a lack of studies to figure out what kind of treatment and cancer site specifically might induce urinary incontinence. Future studies should focus on the investigating association of cancer stage, site and type of treatment with UI in gynecologic cancer patients; and, quantitative evaluation of UI such as a pad test should be performed together with a validated questionnaire. So far, the effects of PFMT in SUI and UUI have been proved in many studies in non-gynecologic cancer. To our knowledge, only two pilot studies investigated the effects of PFMT in gynecologic cancer survivors which resulted to alleviate UI. According to evidence, PFMT had a beneficial effect on controlling bladder and improvement of urinary in gynecological cancer patients as well. In order to have a better result of the training, effects of PFMT on specific gynecologic cancer (e.g. cervical, ovarian etc.) should be concerned. Thus, more research on PFMT exercise intervention study is needed to define the proper frequency, intensity, time and type of exercise related to gynecologic cancer patients’ characteristics.
CONCLUSION
This present study is the first narrative review study to investigate the prevalence of UI in gynecologic cancer patients and effects of the PFMT to increase control of the bladder which will result alleviate of incontinence. This study provides evidence supporting beneficial effects of the PFMT program on improvement of incontinence in non-gynecological cancer subjects and gynecological cancer patients. Thus, we suggest that as a process of rehabilitation of gynecologic cancer patients, the PFMT might be an effective program to treat UI and enhance control of bladder which may improve the overall quality of life in cancer patients.