
INTRODUCTION
Swimming competition and physical activity elevate competition anxiety and the oxygen utility of the body, respectively, leading to, in turn, the elevation of free radical production. Produced free radicals during heavy exercise can damage cells. Vigorous exercise frequently leads to increased permeability of sarcolemma and damage to sarcomeres [1]. One way to determine muscle and cell damage is the measurement of indicators such as lactic acid, Lactate Dehydrogenase (LDH), and Creatine Kinase (CK) [2]. The release of CK from the damaged muscles into the blood is augmented after strenuous physical activity [3]. Plasma CK levels reveal total circulating CK. Thus, post-exercise levels are representative of CK released from damaged muscle tissue [3].
Elevated circulating CK is a marker of damaged muscle [4] that can occur by heavy exercise and is reported in elite Australian Rules football players [5]. A few hours after vigorous exercise, plasma CK elevates, indicated as the prominent indicator of muscle damage. Previous studies have shown that resistance and aerobic exercise modify plasma CK and LDH concentrations [6]. Callegari et al. [7] investigated that the concentration of CK and LDH elevated as ta subsequent consequence of two resistance exercise sessions (multiple sets and bi-sets) and two aerobic exercise sessions (60% and 80% of VO2max). They found that plasma CK and LDH were significantly higher in the post-exercise period compared to the pre-exercise stage. The type of exercises and the length of rest interval between exercise sets can affect the CK concentration in the blood. Another study showed that the plasma CK in the immobilized group was lower than in the control or light exercise groups [8].
Further research showed that a resting period has no significant impact on plasma LDH, but serum CK was significantly affected; therefore, in the group with a long rest period, CK has less concentration. After the futsal game, a significant raising in CK and LDH was detected in plasma samples [9]. Twenty-seven inexpert male individuals completed three sets of 30 maximal isokinetic eccentric contractions of the knee extensors [10]. The log (CK (post)/CK (pre)) looked to be carefully correlated with the relative work lessening (r=0.84).
We have previously shown that plasma lactate levels increase following the Lactate Tolerance Exercise Test [11]. Therefore, this study aimed to compare plasma CK and LDH activities thirty minutes before the lactate tolerance exercise test, immediately, and also twenty-four hours after the test. It was hypothesized that the lactate tolerance exercise test could elevate the plasma concentrations of CK and LDH due to muscle damage.
METHODS
1. Study design
Fourteen male swimmers who were members of a team in Fars province, Iran, had at least 5-10 years of practice experience and were aged 14-18 years, agreed to participate in this study. A longitudinal study design was employed. Subjects who were smokers or users of any nutritional supplements and affected by some types of musculoskeletal diseases were excluded. The swimmers were acquainted with the study’ s aims, procedures, potential risks, and privileges. All swimmers submitted their written consents and formally agreed to participate in this research. This study was approved by the Institutional Review Board (IRB) of Jahrom University of Medical Sciences, Iran (JUMS.REC.1393.016).
A self-selected preparation swimming was done after a resting of 24 hours. Formerly, the participants carried out LTET. This test was counted in an 800 meter (8×100 m) swimming race with greater than thresh-old strength during eight sets using standard diving start at one-minute interset recoveries [11]. The test was done in a 50-meter indoor pool.
Venous blood samples were drawn by antecubital venipuncture from the swimmers, including 30 minutes before LTET, immediately after LTET, and 24 hours after completing the trial set. The blood samples were mixed with ethylenediaminetetraacetic acid (EDTA) in tubes. To obtain plasma, the blood samples were immediately centrifuged on a conventional centrifuge at 1,500×g at room temperature for 10 minutes; then, isolated plasma was kept at -20 degrees Celsius for subsequent laboratory tests. An auto-analyzer analyzed serum CK and LDH levels.
2. Statistical analysis
The Kolmogorov–Smirnov test was utilized to test the normality of each variable. The paired t-test was used to compare plasma concentrations of CK and LDH before LTET with adjustment and 24 hours after the test. The mean and standard deviation (SD) values were calculated for all descriptive variables. A confidence level of 95% or a p-value less than .05 was considered analytically significant.
RESULTS
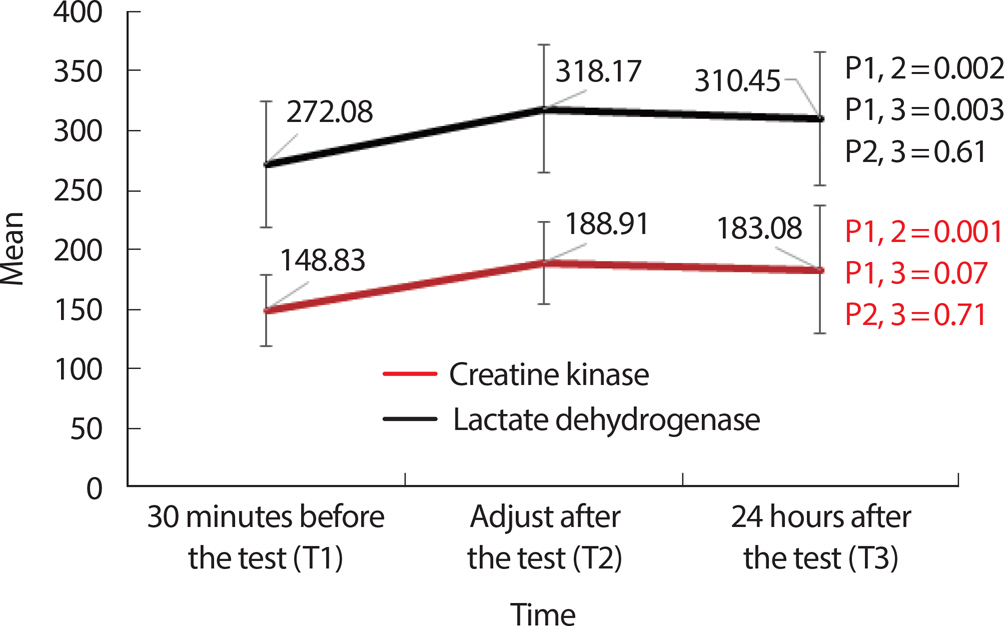
Fig. 1. shows the average level of plasma CK immediately after LTET, which is 27% higher than 30 minutes before LTET (148.83±29.63 vs. 188.91±34.04, p =.001). The mean concentration of plasma CK was also more significant in the 24 hours after LTET than 30 minutes before LTET (148.83±29.63 vs. 183.08±53.84, p =.076). During 24 hours after LTET, the concentration of serum CK reduced to 5.83 mg/dl, but the CK levels did not significantly diminish over time (183.08±53.84 vs. 188.91± 34.04, p =.711).
Our results demonstrated a significant difference between LDH levels before LTET and immediately after the test (p =.002). Also, we observed that the mean level of plasma LDH significantly raised from an initial level of 272.08±52.93 mg/dL before the LTET to 310.45±55.98 mg/dL 24 hours after the LTET (p =.003). According to our results, about 7.7 mg/ dL reduction in plasma concentration of LDH was observed 24 hours after the end of LTET; however, there were no significant differences (310.45±55.98 vs. 318.17±53.89, p =.619).
DISCUSSION
Our study demonstrated a significant increase in plasma CK and LDH immediately after the trial of LTET that diminished insignificantly 24 hours after the test. Barranco et al. [9] showed that serum CK and LDH significantly elevated in eleven futsal players after the game. Meanwhile, after the resistance exercise session in 29 trained women, serum CK activity rose 1.68 folds [12] resemblance to the finding of Thrope and Sunderland in a soccer match [13]. Poprzecki et al. [14] suggested that concentric and eccentric efforts significantly elevated plasma CK and LDH activities, consistent with our results. In contrast to our findings, Mohammadi et al. [15] reported that serum CK and LDH did not increase among four groups at different time points.
It is well established that an increase in CK and LDH activities happens after resistance and aerobic exercise and demonstrates the amount of injury to the membranes of muscle cells [16]. Two types of exercise (downhill running and high-force muscular contractions) showed very diverse CK responses. To exemplify, after downhill running, CK raised from 100 to 600 IU, as the maximum value, within 12-24 hours [17,18]. However, this trend was not seen in CK until about 48 hours after high-force eccentric exercise, with a peak level of generally 2,000-10,000 IU occurring nearly 4 to 6 days after exercise [19].
Plasma CK activity is likely to elevate when eccentric exercise injures more muscles [20], which is changed significantly over time. Liu et al. [21] confirmed that the high-intensity resistance exercise could be pertinent to the higher production of free radicals. Free radicals may interfere with the adaptation of muscle tissues to the functional stress affected by resistance exercise [21]. Through resistance exercise, ischemia/reperfusion in injuries in muscles and the production of free radicals through neutrophils oxidative burst after exercise must be considered the key factors to explain the muscle injury [22,23]. Likewise, mechanical stress is an additional mechanism to elucidate free radical elevation [24]. Specifically, eccentric exercise such as higher force results in muscle tissue damage. This starts the inflammation process, which finally creates the peroxidation of lipid radicals and no oxygen.
Similar to our results, CK activity showed a sustained rising after 24 hours of resting; on the contrary, plasma LDH activity returned to the pre-exercise level [14]. After 7 and 24 hours of recovery, plasma CK level was significantly greater following the eccentric exercise [14]. Meanwhile, Hicks et al. [25] and Moran-Navarro [26], following the 3×10 protocol, observed an elevation of CK activity overtime until 96 hours after an exercise and 24 hours after the end of the protocol, respectively. The augmentation of CK activity was observed in high- and low-intensity resistance exercise groups till 24 hours after ending the exercise [27]. Callegari et al. [7] found that resistant and aerobic exercise increased serum CK and LDH levels after exercise compared to the pre-exercise status. CK elevation continued over time after the ending of practice within 24 hours, which is at odds with our results; even so, LDH levels decreased 24 hours after exercise [7], resemblance to our results.
The discrepancies among the results of various studies are likely to be genetic, exercise protocols, gender of participants, body composition, muscle group involvement, food consumption, etc. [28–33]. Kennekey et al [34]. observed that serum CK levels were higher in 499 African-American subjects undergoing basic training. Amorim et al. [35] suggested that serum CK activity was more significant after an exercise session in males than females. Ravasi et al. [36] found that the resting period after intermittent run training has a significant effect on serum CK; therefore, in the group with a more extended resting period, CK is lower.
In the present study, used markers of muscle damage can be mentioned as a limitation of the study, and it is better to conduct further studies in the future that show muscle damage.


