Comparison of Shoulder Neuromuscular Control in Overhead Athletes with and without Shoulder Hypermobility
Article information

Abstract
PURPOSE
A wider range of motion of shoulder joint is necessary for explosive throwing performance and the increase of the range of motion by repetitive throwing is inevitable. The wide range of motion is related with the instability of the joint. Neuromuscular control plays an essential role in stabilizing the joint. However, when the joint becomes hypermobile, how neuromuscular control was affected was not clear. The purpose of this study was to compare shoulder neuromuscular control of overhead shoulder athletes and identify the influence of hypermobility on it.
METHODS
Total 24 subjects (hypermobility group (HMG); 12 athletes, normal range group (CON); 12 athletes) were recruited in this research. To assess shoulder neuromuscular functions, joint position sense (JPS), the threshold of detection to passive motion (TTDPM), and force reproduction (FR) were measured.
RESULTS
In active JPS at HMG was greater than CON at the 90% target angle, (p<.05). In passive JPS, HMG showed lower JPS compared to CON at the 50% target angle (p<.05). In FR, HMG was lower than CON in internal rotation (p<.05). In relationship test, hypermobility was negatively correlated with active JPS (p<.05).
CONCLUSIONS
It was found that the hypermobile shoulder has greater neuromuscular control compared normal range shoulder to compensate for the hypermobility and active sub-system plays a crucial role in the neuromuscular control of the shoulder joint. Thus, it is recommended that neuromuscular training should be considered in training program for overhead athletes with hypermobile shoulder.
INTRODUCTION
Shoulder joint plays an essential role in throwing performance. Well-coordinated movements of many joints from lower extremities to upper extremities are required for the shoulder performance [1]. In overhead sports, shoulder joint is prone to be hypermobile by repetitive throwing motions with extreme range of motion [2]. The laxity of the joint that can potentially compromise joint stability can be increased [3,4]. Accordingly, during dynamic throwing motion, maintaining shoulder stability is very crucial to produce a greater throwing performance and to prevent injury risks at the wide end range where shoulder is extremely rotated externally [2,5].
The shoulder functions can be influenced by motor abilities like flexibility, stability, strength, neuromuscular control. Above all, joint stability is considered to be fundamental for the other functions of the joint [6]. Joint stabilizing systems consist of 3 sub-systems: passive, active, and neural control sub-systems [7,8]. The passive sub-system provides static joint stability and capsule-ligamentous structures are included in the system. When capsule or ligament is lax, the ability to mechanically support the joint is decreased and it also causes decrease of afferent information of the joint that is transferred to central nervous system (CNS) [9,10]. Active sub-system, including muscles and tendons, is responsible for efficiently producing force and tension for stabilizing trunk and upper extremity [7,11]. Lastly, neural control sub-system provides a considerable interaction between active sub-system and passive sub-system to stabilize the joint [12]. Particularly, in dynamic movement like throwing, neuromuscular control by CNS plays a crucial role in generating appropriate muscle activation to stabilize shoulder joint and produce explosive movements [8].
It has been reported that overthrowing athletes tend to have excessive external rotation of shoulder [2]. The wide range is correlated with greater arm cocking and faster throwing velocity during throwing motion [13]. However, the acquired hypermobility is also considered as the risk of shoulder overuse injuries [14]. It is called as thrower’s paradox that throwing shoulder needs to be mobile and stable simultaneously for maintaining explosive throwing performance and avoiding injury [15].
On the other hand, other researches insisted that the repetitive overhead motions enhance proprioceptive ability of shoulder joint because the repetitive motions near the end range of the joint increase a simulation of muscle spindles in muscles and mechanoreceptors in capsules and ligaments around the joint that is required for joint stabilization [15,16]. However, it is unclear effects of overthrowing with wide range of shoulder motion on neuromuscular function of the joint for throwing performance and injury prevention.
Thus, this study aimed to compare shoulder neuromuscular responses of overthrowing athletes with and without shoulder hypermobility and to identify the influence of hypermobility on neuromuscular response of shoulder joint.
METHODS
1. Participants
Total 24 overthrowing athletes (13 handball athletes and 11 javelins) were recruited and it comprised 16 male and 8 female athletes. The subjects were divided into the 2 groups (hypermobility group [HMG]; 12 athletes, normal range group [CON]; 12 athletes) in this research (Table 1). The active shoulder external rotation was measured. When the external rotation was over 90˚, the participant was allocated in HMG and if less than 90˚ of the rotation, the athlete was allocated in CON [17]. A participant who had a problem on shoulder joint of throwing side and cardiovascular function for last 6 months before this study was excluded from this study. All subjects were informed of the potential risks associated with this experiment before the test. This study was reviewed and approved by the committee on research ethics of Korea National Sport University before all the procedures began.

The characteristics of the subjects in the study
2. Measurements Procedure
1) Procedure
To measure neuromuscular function of shoulder joint in dominant throwing arm, active-and passive-joint position sense (JPS), threshold to detection of passive motion (TTDPM), and force-reproduction (FR) were evaluated in this study. To avoid test errors by muscle fatigue from trials, the order of the tests was as follow; (1) range of motion, (2) AJPS, (3) PJPS, (4) TTDPM, and (5) FR. All tests were performed in shoulder of dominant throwing arm and conducted by same researcher for reliability of test. Isokinetic dynamometer (CSMi, HUMAC, USA) was used for assessing them.
2) Shoulder range of motion (ROM)
In assessment of active ROM of shoulder joint, internal rotation (IR), external rotation (ER), and total range of motion (sum of IR and ER) were measured. The active ROM of shoulder girdle was measured on supine position with 90˚ of shoulder abduction and 90˚ of elbow flexion. When the subjects felt the end feel during shoulder motion, the range was determined as active shoulder range of motion. Two trials were carried out and the average of the results of the measurements was used for the value of range of motion of shoulder joint.
3) Joint position sense
Joint position sense was performed to assess an ability to detect a joint position. Active joint position sense (AJPS) measurement was conducted in the position with 90˚ of shoulder abduction and 90˚ of elbow flexion in supine position. In this study, the target angles were set at 50% angle of the full external rotation and at 90% angle of the end range of external rotation, where joint mechanoreceptors are best stimulated [18]. First, the subject was held at the target angle for 5 seconds by the instructor and then asked to memorize it. After returning to the start position, the subject was instructed to reproduce the target angle and to say “STOP” when they feel the joint is reached at the target angle [19]. Passive joint position sense (PJPS) was also assessed on same position with AJPS [18]. The subject was only instructed to passively replicate the target angles. The 2˚/sec velocity of passive movement was used in PJPS. Total 3 tests were performed after 2 practices and 10 seconds were provided between trials for rest in AJPS and PJPS assessments. Error angles between target angle and reproduced angle were recorded as the value of the tests. The average of 3 error angles was recorded for the result of the measurement. Each participant wore blindfold, headset with white noise and pneumatic sleeve to eliminate visual, auditory and tactile afferent information from the measurement device [20].
4) Threshold To detection of passive motion
TTDPM is a method to evaluate an ability to sense a slow passive motion of joint. TTDPM was also assessed on same position with JPS and on internal- and external rotations. The velocity of the passive motion was set at 0.2˚/sec. The test arm of the subject was passively moved to the start position, at 45% angle of the range of external rotation and the subject was asked to say “STOP” as soon as it perceived the passive motion. 2 practice trials and 5 tests, and 10 seconds break for rest among the trials were provided [21]. The displacement between the starting angle and the perceived angle was recorded for the result of the trial. The average of the 5 results was recorded for the result of the measurement [22]. In TTDPM, blindfold, headset and pneumatic sleeve were used to eliminate the afferent information [20].
5) Force-reproduction
FR was carried out to assess the ability to sense tension or force produced in a joint [23]. FR test was performed in standing position with 45˚ of shoulder abduction in the scapular plane and 90˚ of elbow flexion. Firstly, maximum voluntary isometric contraction (MVIC) of internal rotation of shoulder was measured. 3 measurements of MVIC were conducted and 50% of the highest MVIC was used for the target force to reproduce [18,23]. For FR test, we instructed the subjects to maintain 50% torque of their highest MVIC in shoulder IR for 3 seconds. to perceive the force. Participants were asked to replicate the target force for 3 secconds. and to express verbal sign, ‘stop’ when they perceived the target rotational moment. Before testing, visual and audible feedbacks were removed by blindfold and headset. The subjects had 2 practices and 3 measurement trials. 10 seconds break time between trials was provided for resting. The force difference between the target force and reproduced force was calculated at each trial and the average of the measured forces was determined for the test results [22].
3. Statistical Analysis
The data was analyzed by SPSS program (version 18, SPSS INC, Chicago, IL). All values were presented as mean and standard deviation (mean±SD). Independent t-test was performed to compare AJPS, PJPS, TTDPM, and FR of hypermobility group and normal range group. Pearson correlation analysis was used to analyze a relationship between hypermobility and neuromuscular responses in the throwing shoulder joint. The relationship’s strength was identified follow as; 0.00-0.25=little or no;0.26-0.50 =fair; 0.51-0.75 =moderate to good; 0.76-1.00 =good to excellent. Statistic level of less than 0.05 was considered significant.
RESULTS
1. Shoulder range of motion
In shoulder ROM, hyper-mobility group HMG significantly demonstrated greater compared to normal range group (CON) in external rotation [HMG (102.83˚±7.61) vs. CON (74.17˚±4.02˚), p=.000] and total range of motion [HMG (161.83˚±18.33˚) vs. CON (130.42˚±7.77˚), p=.000]. There was no significant difference between HMG and CON in internal rotation of shoulder [HMG (59.00˚±13.06˚) vs. CON (56.25˚±7.30˚), p=.637] (Fig. 1).
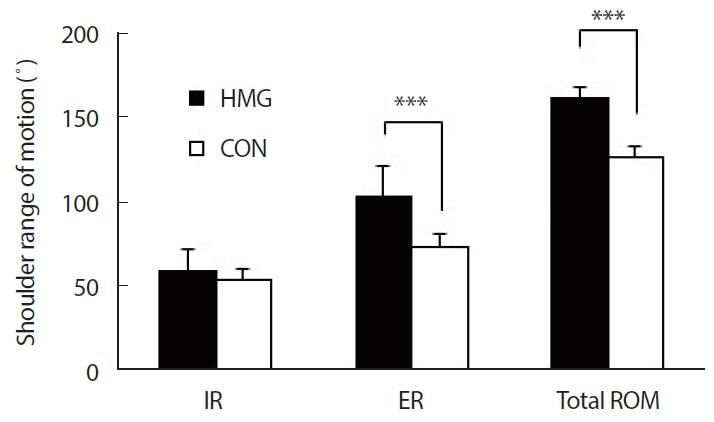
Range of motion (ROM) of shoulder joint in the groups. HMG; hypermobility group; CON, normal range group; IR, internal rotation; ER, external rotation; Total ROM, total range of motion. *HMG vs. CON; ***p<.001.
2. Joint position sense
JPS was assessed at the 50% and 90% angles of the range of shoulder external rotation. In AJPS, hyper-mobility group showed less error angles than control group at the 90% target angle, (p=.043). On the other hand, at the 50% target angle, it was shown that there was no significant difference between the both groups in AJPS (p=.075). In PJPS, no significant difference between HMG and CON at the 90% target angle was appeared (p=.055). However, at the 50% target angle, hypermobility group showed greater error angles compared to normal range group in PJPS (p=.035)(Table 2).

JPS, TTDPM and FR of shoulder joint in the groups
3. Threshold to detection of passive motion
TTDPM was also evaluated at the 45% of the range of external rotation to perceive passive motion of shoulder joint. The result showed there was no significant difference between HMG and CON in TTDPM to detect passive external rotation of the joint (p=.321)(Table 2).
4. Force reproduction
In this study, force reproduction test was performed to evaluate an ability of mechanical feedback of muscles around shoulder joint. The result was shown that the force reproduction ability of HMG was lower than that of CON in internal rotation (p=.013)(Table 2).
5. Hypermobility and neuromuscular control
Hypermobility seemed to be negatively related with error angles of AJPS at the 90% target angle (r=-0.416, p=.043)(Fig. 2). However, there was no significant relationship between hypermobility and error passive joint position sense (at 90%ER, r=.052, p=.811; at 50%ER, r=.298, p=.157). Hypermobility was also positively correlated with force production (FR) ability in internal rotation (r=.533, p=.007). Relationships between hypermobility and TTDPM was not significant (r=.260, p=.220).

Relationship between shoulder external rotation and active joint position sense.
DISCUSSION
The purpose of this study was to identify relationship between joint hypermobility and neuromuscular control of throwing shoulder. Shoulder joint plays a key role in throwing performance in the sports such as baseball, volleyball, handball, and javelin [1]. Muscle strength, flexibility, stability, and power are required for the explosive motion [6]. However, repetitive throwing motions in games and practices can make a shoulder joint lax and hypermobile. As a result, it causes instability of the joint [3]. The stability should be maintained for throwing performance and injury prevention during the dynamic motions [5]. A neuromuscular control is necessary for a joint stabilization in the wide range of motion [16].
In this research, HMG showed greater external range of motion in shoulder joint compared to normal range group (CON). Generally, a range of motion of throwing shoulder tends to be greater than the range of non-throwing side and it is usually referred to as ERG [15]. In previous studies, it has been reported that in overhead sports, a hypermobility of the dominant throwing shoulder has been steadily observed [24]. However, the fact is controversial for years whether the acquired joint motion is required for throwing performance or needed to be controlled for preventing an injury [13,14]. Some researchers have insisted that maintaining the stability in the wide range is important for the both goals during dynamic motion like overhead throwing [25]. Joint stability is determined by a mount of stiffness of soft tissues such as capsules, and ligaments and neuromuscular function [7,8]. Hence, in this study, joint position sense TTDPM, and force reproduction (FR) were measured to identify neuromuscular function of shoulder joint.
JPS is the neuromuscular function to detect joint positions and JPS can be conducted in active and passive modes [19]. AJPS is to evaluate an ability to perceive joint positons during dynamic motion [20]. Dynamic stabilization system, like active joint position, is a key function to stabilize and control a joint during mid-range of joint motion [26].
In AJPS test, HMG group showed higher joint position sense than CON group. The result observed is consistent with other researches reporting that hypermobile joint groups or subjects are inclined to have greater neuromuscular functions compared to normal range groups [27,28]. In the correlation between hypermobility and neuromuscular function, it was also found that hypermobility was natively related with errors of active joint position sense. It means that the more hypermobile shoulder is inclined to have greater neuromuscular function in overhead throwing athletes. For explosive throwing performance, overhead athletes require a sufficient range of motion of shoulder joint where can efficiently produce greater force from stretched muscles of shoulder joint in terms of length-force relationship [29] and simultaneously, joint stability needs to be controlled within the wide range during the explosive overhead motion [23].
Additionally, when the joint is approached to the end range of joint motion during throwing, mechanoreceptors in muscles, capsules, ligaments, and fascia are stimulated [10], overhead athletes are able to take advantage of greater stretch-shortening cycle (SSC) reflexively produced by the stretch-induced stimulation for power production. In addition, at the end range, afferent input transferred to CNS for controlling the joint is also increased [30]. Hence, in overhead sports, neuromuscular control of hypermobile shoulder should be well-trained and adapted to the dynamic throwing motion for better performance and injury prevention during the wide range of motion.
However, HMG group showed greater joint position errors than CON group in PJPS that in passive mode. It means neuromuscular function of hypermobility group is lower than normal range group in passive mode to assess mainly proprioceptors stimulated passively [19]. This finding results from the effects of increased joint laxity acquired from repetitive throwing motions.
TTDPM, greater errors in HMG group were found compared to CON group, although there was no significant difference between the both groups. Furthermore, in the correlation analysis, hypermobility was negatively related with passive joint position sense at 50% target angle where muscles around the joint are relatively less stretched and loose. The results can be explained by changes of the afferent information discharged from mechanoreceptors of the shoulder joint [31].
Joint laxity is mainly determined by passive sub-system like joint capsule and ligaments [7,32]. Since the capsule-ligamentous structures are loosened, joint laxity is increased and then the joint is able to be hypermobile and instable [33]. A tension in the loosened tissues is decreased and then the afferent information transferred to central nervous system is also reduced [34]. As a result, decreased neuromuscular function such as joint position sense and kinesthesia of shoulder joint from the laxity causes joint instability during the dynamic motion [35]. Due to the aforementioned reasons, in overhead throwing athletes with shoulder hypermobility, shoulder muscles like rotator cuff, play an important role in actively controlling the joint stability during wide range motion [36]. Therefore, neuromuscular training should also be included in the training program for overhead sports athletes who have hypermobile shoulder with strengthening muscles [37].
FR test was used to evaluate an ability to regenerate the muscle force that the subjects produced before [18,23]. FR test is known as a modality to assess the sense of tension that comes from mechanoreceptors embedded in muscles [38]. When muscles around joint are stretched near the end range of the motion, activation of muscle spindles and additional tension from ligaments and capsular structures of joint are increased for dynamic stabilization of joint [31]. It is helpful for detecting a sense of force and tension of the joint [39].
In the FR test of this study, the force reproduction ability of HMG group was lower than CON group. It means that a change of muscle stiffness alters amount of afferent information from the muscle spindle and joint mechanoreceptors. The alteration of the proprioceptive information affects the ability to sense force produced at the target joint angles [40].
The results of the FR test can be explained by the change of muscle stiffness. It is influenced by the testing position, 45 degrees of shoulder abduction in scapular plane. At the position, the anterior muscles of the shoulder joint of HMG group were relatively less stretched and loose compared to CON group. The decreased tensions by the loose muscles can affect a detection of the muscle sense produced in the joint. In previous study, it was reported that a difference of muscle tension influences on the ability to detect tension by muscles of joint [23]. Thus, to accurately measure the ability to sense a tension and force of joint, the ability is need to be assessed at various joint angles or muscle lengths [41].
As a result, the wide range motion of shoulder joint, especially in external rotation, is inevitable and natural phenomenon for throwing performance. To get the wide range of shoulder, the shoulder joint should be flexible and stable for explosive movement. Thus, muscle function and neural control are important for maintaining stability of shoulder joint for throwing athletes. In this study, it was found that hypermobile joint group has greater neuromuscular function controlled by active subsystem than normal range group but in passive motion, neural function of hypermobility group was lower compared to normal range group. It means active sub-system like muscle plays a more crucial role in neuromuscular function of shoulder joint in the dynamic overhead throwing. Neuro-muscular functions like sensitivity or reflexive response of muscles around throwing shoulder should be considered and included in training and conditioning program for throwing performance and joint stability of overhead throwing athletes.
However, in this study, measurements about throwing performance were not conducted. So it is unclear how difference of neuromuscular control in shoulder joint influences on throwing performance. In the future research, the research that identifies influences of neuromuscular function on throwing performance in overhead athletes with hypermobility will be needed. Also, small number of overthrowing athletes were recruited in this study. The numbers would be not enough to clearly identify the effect of shoulder hypermobility on neuromuscular control of the overhead throwing joint. Future research should therefore be conducted by greater number of overhead athletes.
In conclusion, throwing shoulder should be mobile to throw it explosively and stable to prevent an injury from repetitive overhead motions. The present study investigated the influence of the shoulder hypermobility on neuromuscular control in overhead athletes. It was found that the hypermobile shoulder has greater neuromuscular function than normal range group in dynamic motion test. It means the greater neuromuscular control in hypermobile shoulder is appeared to compensate for the hypermobility and active sub-system like muscle, plays a crucial role in the neuromuscular control of the shoulder joint. Thus, it is recommended that neuromuscular training should be considered in training program for overhead athletes with hypermobile shoulder. Future studies on relationship among hypermobility, neuromuscular control, and throwing performance will be informative to improve a throwing performance and prevent a shoulder injury.
Notes
No potential conflict of interest relevant to this article was reported.
AUTHOR CONTRIBUTION
Conceptualization: SWK, KLK; Data curation: SWK; Formal analysis: SWK; Funding acquisition: KLK; Methodology: SWK, KLK; Project administration: SWK, KLK; Visualization: SWK; Writing-original draft: SWK, KLK; Writing-review & editing: SWK, KLK.
Acknowledgements
The author appreciates the subjects for participating in this study. This research was supported by the Hanyang Women’s University Research Grant 2018 (2018-2-012).