
INTRODUCTION
Physical activity is an important factor that can reduce mortality rate and improve the health and welfare of older adults (65+ years) [1]. Regular exercises are needed to prevent impaired balance and gait function loss attributable to less physical activities and physical dysfunction caused by the normal aging process in aged people with senility [2,3]. American College of Sports Medicine (ACSM) has recommended ordinary aged people to have exercises, including aerobic exercises, muscle strength/endurance exercises, and flexibility exercises [4]. It has insisted that exercises can improve balancing capability, agility, and proprioceptive capability for those who frequently experience falls or having limited mobility. Aged people are also advised to take care of weight bearing exercises causing orthopedic stresses. Thus, exercises such as swimming and bicycling are recommended for aged people because they are less weight bearing with less physical and mental stresses [4].
In particular, walking is better than mountain climbing or running for aged people because it is safer and more adequate in that it gives them less articular stresses than aerobic exercises [5]. For aged people, light exercises such as walking (ex. HRmax 40-60%, VO2max 35-40% maintain) are more effective than highly intensive exercises to increase the level of their independent physical activity through improving their degraded physical functions such as cardiopulmonary function, muscle strength of the lower and upper extremities, muscle endurance, and articular flexibility [6,7]. However, walking exercises performed on hard ground surfaces might lead to plantar fasciitis, rheumatoid arthritis, and reactive arthritis in aged people because shocks of the exercise can transfer directly to the sole of the foot [8,9].
Compared with general training surfaces, such as playground, there are distinct physiological and biomechanical differences associated with sand exercise. These include significant alterations in kinematics and muscle activation patterns when running on sand contributing to significantly greater energy expenditures than at similar running speeds on hard surface.
In addition, it has been reported that exercises on sands can reduce the risk of exercise injuries and improve proprioceptive sensibility attributable to the neuromuscular adaptation [10]. Exercises on sands can also bring various kinematic, neuromuscular, and physiological changes through improved aerobic capability, agility, and myopachynsis [11-15]. Sandy surface causes less post exercise myalgia than hard ground surface [16,17]. It consumes more exercise energy of players [12,13,18-20]. Thus, exercises on sands are recommended to improve both aerobic- and anaerobic exercises [13,18]. It is used in rehabilitation for neuromuscular injuries [10,12].
Recently, tools providing an unstable ground surface filled up with air, such as BOSU® ball (Hedstrom Fitness, Ashland, OH, USA) and DynaDiscs® (Exertools, Inc, Petaluma, CA, USA) are occasionally used. However, these are static ones with limitations for an application program. The surface of sands on a beach can embrace not only static exercises, but also diverse dynamic ones [16,21]. Like this exercises performed on sands can compensate such problems of exercises on hard ground surfaces.
Whereas consideration should also be given to the effects of sand surfaces on injury prevalence. Previous research is equivocal, with reports that exercise on sand can either increase [22] or decrease injury incidence [16] compared with firm surfaces. The unstable and shifting nature of a soft, dry sand surface is generally thought to increase the risk of musculoskeletal injury in the lower extremity [23]. In contrast, firmer training surfaces are associated with a higher incidence of impact-related [24], and overuse injuries [25].
Therefore, it could be argued that the lower impact forces experienced on sand could ultimately decrease the risk of injury, and the overall physical strain to a given training session [26]. Exercises performed on sands can compensate such problems of exercises on hard ground surfaces.
Despite such suggestions, there is currently a lack of evidence investigating the long-term effects of training on sand, and the implications for general ground performance gains. Additionally, domestic and overseas prior studies on such topics have reported various effects of exercises on unstable ground surfaces. However, these studies have focused on limited elements to improve athletic ability of athletes [11-13,18,20,27]. Studies focusing on exercises on sands for ordinary people are few. In particular, studies delved into effects of exercises on sands for the elderly are rare.
As such, a greater understanding of sand training is necessary to fully gauge the extent of its application to training methods. Therefore, the aim of this study was to effects on sand training, with a specific focus on its potential use as an alternate training venue for elderly people.
The objective of this study was to provide new ways of exercises for aged people to prevent them from loss of physical function owing to the normal aging process in their senility, focusing on effects of exercises on sands on muscle strength of lower extremities, inflammatory indicators, balancing capabilities, and muscular activity of older women.
METHODS
1. Subjects
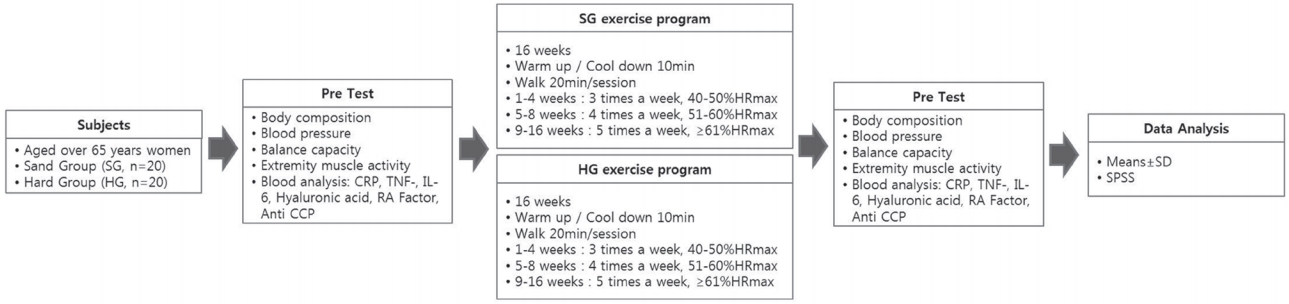
A total of 40 people aged over 65 years women living in the district under the “Health Center B” were selected as subjects of this study. These subjects were informed about the purpose of this study. Those who provided consent to plans provided in this study were selected and randomly classified into two groups (20 subjects in each group): 1) exercises on normal ground surface; and 2) exercises on sands. Exclusion criteria were: 1) recent drug use that could potentially affect test results, 2) the presence of cardiovascular diseases in recent 5 years, 3) the presence of physical problems due to medical operations or severe arthritis that could disturb physical exercises, or 4) the presence of regular aerobic exercises during recent three months. The characteristics of the study group are described in Table 1.
2. Exercise program
The maximal heart rate was calculated with the following formula: HRmax=220-Age. It was applied to exercise programs. The heart rate of each subject was monitored continuously during the exercise using a wireless heart rate measuring instrument. Exercise programs on sands were carried out 20 minutes per session for 16 weeks on the beach. Exercise programs on normal grounds employed racetrack in a park. These two groups followed exercise programs designed to increase the intensity of exercises gradually, including the following: 1) 3 times/week of exercises for 20 minutes in each session from the 1st week to the 4th week at 40-50%HRmax; 2) 4 times/week of exercises for 20 minutes in each session from the 5th to the 8th week at 51-61%HRmax; and 3) 5 times/week of exercises for 30 minutes in each session from the 9th to the 16th week at >61%HRmax. Free walking and stretching of body for 10 minutes were taken as warming-up and cooling down, respectively.
3. Assessment procedures
The diagram of study design are described in Figure 1.
Subjects found eligible based on the selection criteria underwent examinations of height, weight, BMI (Venus 5.5, Jawon Medical Co., Korea), and blood pressure (an average from the two measurements; Jawon Medical Co., Korea) after resting 10 minutes in seated position.
Balance System SD (Biodex, USA, 2009) was employed to test the balancing capability of subject. The equipment consisted of a “balance plate (platform)” and a “displaying unit”. It had 12 strain gauges in the platform to measure the balance plate and angle of inclination. The balance plate can be tilted up to 20° in every direction. The tilted angle was used to represent the level of stability of static balance. The score for balancing capability was comprised of scores for antero-posterior/postero-anterior balancing, lateral balancing, and overall balancing, with lower scores of the balance plate and angle of inclination indicating better stability. For the examination, subjects kept an orthostatic posture on the base plate to obtain three measurements. The experimental process was carried out following programmed instructions shown in the displaying unit.
To measure proprioceptive sensibility, CSMi (Humac, USA), an isokinetic device, was used. The proprioceptive sensation of knee joint was measured. For this measurement, two eyes of the subject were blinded. The subject remained in a state of null resistance. From the starting angle of 90°, target angles set 15° and 45° were kept respectively for 10 seconds for the subject to remember respective angles. After the duration of 10 seconds, the knee joint of subjects returned to its initial position and the subject was asked to find the memorized angle spontaneously. Three respective measurements were taken from each subject. After excluding the one with the greatest error from the set target value, the average value from the remaining two measurements was calculated.
Biodex system III (Biodex Medical Systems, Inc., NY, USA) was used to test muscle strength of lower extremities of subjects. For this test, concentric-eccentric contraction (Quadcon, Hamecc) and eccentric-concentric contraction (Quadecc, Hamcon) of the talocrural joint (30°/sec, 120°/sec) and knee joint (60°/sec, 180°/sec) were measured, respectively. To find the level of muscle activity of the subject, measurements of superficial electromyogram (Noraxon, MyoSystem 1400A) were used. Ag/AgCl electrodes situated at each position placed within 20-mm distance from each other were used. These electrodes were attached to the tibialis anterior, the gastrocnemius, and biceps femoris of dominant legs of the subject. The active electrode was arranged parallel to the direction of muscle fiber in the middle of muscle. Root mean square values of the amplitude of signals of electromyogram of 30 seconds were taken for analysis. Signals continued for 24 seconds were taken after discarding unstable signals of the initial and final 3 seconds.
All subjects arrived at the laboratory of D-University at 9 o’clock in the morning for blood test after fasting for 10-hours without excessive physical activities. These subjects then took rest respectively for blood collection (10 mL) from the cardinal vein of the forearm. Time points for blood collection were: 1) before taking exercises, and 2) 16 weeks after taking exercises. Collected blood samples (human materials) were forwarded to “Green Cross” for blood examination. Levels of C-reactive protein (CRP), tumor necrosis factor-α (TNF-α), and interleukin-6 (IL-6) as inflammatory markers of the knee were measured. Hyaluronic acid, a rheumatoid arthritis factor, and anti-cyclic citrullinated peptide were taken as rheumatic inflammatory markers. These were analyzed using Human ELISA Kit (Enzyme-linked immuno-sorbent assay; ELISA, R&D Systems, Minneapolis, MN, USA).
4. Statistical analysis
Data analysis was performed IBM SPSS Statistics for Window Version 20.0 (IBM Corp., Armonk, NY, USA). All data were expressed as the mean and standard deviation. Two-Way ANOVA was used to control for difference between groups, test periods, body composition, and balancing capability, proprioceptive sensation, Muscle activity, inflammatory markers changes caused by different surface exercise type, and the paired and independent t-test method was used for the post hoc test. A level of statistical significance of p<.05 was adopted for this study.
RESULTS
There was no interaction effect between group and time on body composition and blood pressure. Body composition and blood pressure of subjects in both groups appeared to be decreasing after taking exercises than those before taking exercises. However, no statistically significant differences were found between the two groups (Table 2).
There were significant difference in overall, anterior/posterior, medial/lateral between the SG and HG (p<.05, respectively). Changes in balancing capability of subjects showed significant differences between the two groups (p<.05, respectively) (Table 3).
Changes in measurements of proprioceptive sensation collected from examination for active articular position sensation at 45° showed statistically significant differences between the two groups (p<.05) (Table 4). For subjects with exercises on sands, changes in measurements of proprioceptive sensation collected before and after taking exercises were also statistically significant (p<.05).
For changes in muscle strength based on measurements collected preand post-exercise, there were statistically significant differences in changes of muscle strength of knee extension between the two groups (p<.05). Knee extension was also significantly higher in the HG than in the SG (p<.05). Subjects of both groups commonly showed increase in muscle strength after exercises (Table 5).
Muscle activity was compared by using pre- and post-exercise measurements for the tibialis anterior, the gastrocnemius, and biceps femoris of each subject. There were significant difference in the tibialis anterior, the gastrocnemius, and biceps femoris between the SG and HG (p<.05, respectively). There were significant increases in respective muscle activities after exercises in SG (p<.05) (Table 6).
There was no interaction effect between group and time on inflammatory markers. After the exercise program, there was a significant difference between times in CRP (p<.05). There were significant difference in C-reactive protein between the pre and post in SG group (p <.05). There were significant difference in RA factor between the SG and HG (p<.05). Also, SG resulted in a greater reduction in RA factor than the HG (p<.05) (Table 7).
DISCUSSION
This study was designed to provide new ways of physical exercises and programs for aged people to avoid the loss of physical functions due to less physical activities and physical dysfunction attributable to the normal aging process in senility. The study also intended to identify effects of exercises on sands on muscle strength of lower extremities, inflammatory indicators, balancing capability, and muscle activity of aged people obtained through various inputs of somatic senses and stimuli of proprioceptive sensation.
In general, normal step velocity and cadence for males are 101-133 cm/sec and 94-110 steps/min, respectively. For females, they are 96-136 cm/sec and 93-133 steps/min, respectively. For the elderly, a decrease in step velocity by 10 cm/sec would be equivalent to 10% decrease of mobility in daily living. This signifies the importance of muscle strength of lower extremities for aged people [28].
In this study, subjects with exercises on sands were found to have increased muscle strength more than those with exercises on normal ground surface. Pinnington et al. [18] have compared muscle activity of the gastrocnemius before and after taking running exercises on lawn ground or on sands. They found that subjects after running exercises on sands showed further increase in muscle activity of gastrocnemius due to significant increase of (ankle joint) plantar flexion.
Morrison et al. [20] have reported that knee strength of female subjects aged of 60 to 75 years is improved after physical exercises on hard ground surfaces or sands. However, those with exercises on sands had larger effects than those with exercise on hard ground. Although exercises on normal ground and sands commonly improved physical capability of participants, exercises on sands resulted in further improvement in terms of physical capability. Additionally, Pinnington et al. [29] that there is significantly greater electromyographic activation of the lower limb muscles when running on sand compared with on grass, due to increased stabilization demands around the ankle, knee and hip joints. Such result is attributable to characteristics of sands. It is known that sands can absorb shocks or kinetic movement, eventually requiring significant dynamic balancing capability and more energy consumption for ankle joint of players to complete further diverse movements on sands, thus demanding more muscle strength [10]. This suggests that exercises on sands could result in greater stimuli for certain muscles compared to exercises on an ordinary hard ground surface. Proponents of unstable devices suggest that the greater instability may stress the neuromuscular system to a greater extent than stable surface [30,31]. The rationale is that destabilizing training environments may enhance neuromuscular adaptations and training specificity, while providing a more varied and effective training stimulus.
The Canadian Society for Exercise Physiology position stand [32] indicates that there are functional health benefits of unstable surface (e.g. improved joint stability and reduced lower-extremity injury rates). In addition, improved strength, balance and functional performance have been reported following unstable surface in primarily young healthy adults [33]. Further, unstable surface appears to be a suitable training regimen to be implemented in the rehabilitative context and/or the geriatric context [34,35]. In fact, the application of unstable surface is not restricted to young healthy adults. For example, more ‘vulnerable’ cohorts due to biological aging (i.e. seniors) or maturational processes (i.e. children, adolescents) may particularly benefit from STU because surface instability allows and demands lower training loads but at the same time sufficiently and adequately stimulates the neuromuscular system of youth and seniors [32,34,36]. However, Given that only a few studies have investigated the effects of sand surface as a promising training regimen in seniors, more research is needed to elucidate the effects of sand surface in seniors and to find out whether it is more effective than traditional general surface.
There was further improvement in muscle activity for subjects with exercises on sands compared to subjects with exercises on hard ground. In particular, muscle activity of tibialis anterior and the soleus of subjects with exercises on sands showed significant improvement commonly after exercise. However, muscle activity of the soleus in subjects with exercises on sands was improved further than that in subjects with exercises on ordinary hard ground.
This result might be attributable to consequential kinetic output increased eventually by the muscle spindle sensitized through the gamma motor neuron activated by walking on unstable bearing surface of sands [37]. Exercises on sands may give participants diverse sensory experiences. Thus, consequences of such exercises may appear with undetermined patterns with floating variable. Physical exercises can give diverse stimuli to the body of participants. The ability of sands to absorb or buffer shocks created by physical exercises makes exercises on sands a unique means for rehabilitation and physical training of the lower extremities.
In this study, subjects with exercises on sands were found to have more improvement in balancing capability than those with exercises on normal hard ground. Exercises on unstable bearing surface like that of sands might be effective ways to strengthen muscles and train proprioceptive sensation [38].
Different from walking on normal hard ground surfaces, walking on sands might improve muscle strength of legs of subjects through motions required to achieve movements of the center of gravity of their bodies laterally or back and forth on sands by keeping balances. For this, the input of somatic sensation might have also increased accordingly, resulting in improvement of the proprioceptive sensation crucial to the improvement of muscle strength.
Gait training on unstable ground instead of firm ground requires more diverse movement in the ankle joint as well as large muscle strength [36]. Using such environmental characteristics can induce greater ankle mobility and improvement of proprioception.
For aged people, the exercises on unstable bearing surfaces like those of sands should be kept continuously under long-ranged plans taking such exercises as a means to improve their static or dynamic balancing capability [39]. In this study, exercises on sands intended to improve muscle contraction of the lower extremities of participants by loading their body weight on their lower extremities on specific condition of the surface of sands.
As results of such exercises conducted in this study, the muscle strength of lower extremities of subjects was improved together with improvement of muscle activity and proprioceptive senses, resulting in improved balancing capability that could prevent aged people from potential falling injuries. The improvement of proprioceptive sensation through facilitation of diversified movement of ankle joint is known to be effective for improving muscle strength of ankle joint, balancing capability, and walking [26]. Changes in proprioceptive sensation inputted through the sole of the foot could help keep balance of body and improve balancing capability.
The results of this study showed that walking on sand has the potential to reduce the resultant inflammatory markers relative to matched exercise intensities on a hard surface.
Different from exercises on soft ground surfaces, exercises on hard ground surfaces may cause problems of plantar fasciitis, rheumatoid arthritis, or reactive arthritis due to shocks transferred directly through the sole of the foot [8,9]. Exercise on sands would not only compensate such health problems, but also diminish the risk of exercise injuries while improving proprioceptive sensation by neuromuscular adaptation [10].
Exercises on sands can also bring diverse kinematic, neuromuscular, and physiological changes due to improved aerobic exercising capability, agility, and myopachynsis [11-15].
In previous studies, muscle soreness rating of subjects with exercises involving equal contacts of feet on sands has been found to be decreased on the day after exercises compared to subjects with exercises on hard ground surface [16,17].
Another study has also reported that the level of myoglobin (Mb) is significantly increased in subjects with exercises on lawn ground compared to that in subjects with exercises with equivalent intensity and duration on sands. Post-exercise acute reaction of Mb implies that the degree of muscular damage is increased further by exercises on lawn ground surface [27].
Such consequences might be attributable to the characteristic of sands that can absorb shocks adding to the ground surface. To support the presumption above, surface strength of sands and lawn ground against the exercises was measured. Results showed that the impulse on lawn ground was 3.8 times bigger than that on sands. With this discovery, exercises on sands have been reported as a means to reduce muscular injuries of players because sands can reduce impulses related to training exercises [13,18].
Therefore, under equivalent condition of exercise intensity, exercises on sands can be presented as a means to reduce muscular injuries of players who have been trained on traditional (lawn) ground surfaces. By summarizing results obtained from prior studies, sands could produce less muscular pain for players compared to hard ground surfaces [16, 17].
Previous research has shown that higher muscle contraction velocities result in greater muscle damage [40]. Therefore, altered walking on sand may have resulted in slower contraction velocities which could explain the differences in muscle damage observed here. Although possible, this study was primarily focused on matching exercise intensity and time, and therefore, even if a greater degree of muscle damage was the result of altered running kinematics, an attenuated blood marker response for an equivalent training intensity stimulus was still the primary outcome.
Consequently, these outcomes may in fact suggest that a matched training intensity between ground surfaces could result in lower relative degrees of muscle damage and inflammation, as myoglobin and C reactive protein are well-known markers of muscle damage and systemic inflammation, respectively, and have been shown to be sensitive to exercise intensity.
Perhaps, future research could examine differences in walking kinematics at a variety of matched exercise intensities on both sand and hard to determine its impact on muscle damage.
Taking sands as a surface for exercises can accommodate players of dynamic exercises as well as players of static exercises [16,21]. Therefore, exploitation of sands for exercises could prevent falling injuries and muscular loss of aged people owing to aging in their senility. It will also improve their muscular strength. Such exploitation could be very important because such improvements are related to their quality of life.
This study is significant in that a new application program that could compensate results of recent studies that tested the effect of exercises on diverse types of grounds is presented. The unstable surface of sands was found to have beneficial effects for aged people after exercises. This could contribute to prevention of arthritis and improvement of muscular activity by increasing muscle strength of the lower extremities of aged people.
Therefore, sand has the potential to not only offer a unique training stimulus for older people, but this training surface might also be considered as a viable option for recovery and rehabilitation sessions.
The protocol presented in this study can be employed as a general exercise program for aged people or a rehabilitation program for patients. Broad application of such programs is thus expected in that it could prevent aged people from frequent injuries of falling, consequently improving their quality of life.
CONCLUSION
Our results suggest that sand exercise program can produce benefits with regard to balancing capacity functional improvement, reduction of inflammatory markers, and prevention of proprioceptive sensation in the older women, thus contributing to a better quality of life.
However, to conclusively confirm these benefits, investigators need to conduct randomized controlled studies with large subject samples and better assessment conditions. In addition, there may be differences according to the training of barefoot walking in the experimental group and the wearing of the sneakers during the gait training of the control group. Therefore, future studies need to be compared under the same conditions.