
INTRODUCTION
Medial tibial stress syndrome (MTSS), a term that related to exercise related leg pain, shin splints, or stress fractures, is one of the most common overuse lower leg injuries among runners and military personnel [1]. Previous studies have reported that MTSS accounts for 6 to15 percent of all running related injuries [2,3]. In addition, a high incidence of this injury was observed in military recruits of whom up to 35 percent developed MTSS [1]. This condition is characterized by a pain along the distal posterior-medial aspect of the tibia [4].
Due to the high incidence of this injury, many prospective and retrospective studies [5-12] examined many suspected kinematic risk factors for overuse leg injuries during gait cycle. However, the findings from these previous studies are controversial results. Even though these previous literatures examined kinematic variables including ankle, knee, and hip joint, some studies [1,10,13-15] found the significant relationship between lower extremity alignment (e.g., foot posture; pronation) and overuse leg injuries. Based on these findings, this review paper focused on ankle joint kinematic variables to confirm whether there is a relationship between pronation and overuse leg injuries during gait or not, since a relationship between alignment and overuse leg injuries was found.
Numerous studies [8,9,11,12] found that kinematic variables of rearfoot and tibial motion such as peak rearfoot eversion, maximal foot abduction, eversion/abduction excursion, maximal eversion/abduction velocity in overuse leg injury group were greater than the healthy leg group. On the other hand, similar studies [5-7] identified that there was no significant difference on kinematic variables of rearfoot and tibial motion between overuse leg injury and healthy group. As reported above, the kinematic risk factors of overuse leg injuries exist in the previous literatures but inconsistent and conflicting results were found. However, kinematic variables of rearfoot and tibial motion from previous studies are related with the deviation of the subtalar joint axis that influences subtalar joint motion in the frontal and transverse planes. The subtalar joint axis is deviated about 41º to 42º from transverse plane [16]. This normal deviation produces the pronation of rearfoot is a triplanar motion in the closed kinetic chain and is a combination of adduction and plantar flexion of the talus and eversion of the calcaneus, which causes internal rotation of the tibia [17]. Excessive pronation can increase tibialis posterior tension at the periosteal interface that results in leg overuse injuries such as shin splints, MTSS, and stress fractures [18].
Thus, the purpose of this paper was to determine if rearfoot and tibial motion are associated with overuse injuries during gait. It was hypothesized that individuals with overuse injuries might have a more subtalar joint motion in the frontal and transverse planes. The finding of this systematic review study will confirm the risk factors associated with MTSS during gait and enable the clinicians to develop evidence-based prevention and rehabilitation programs for runners.
METHODS
1. Search strategy
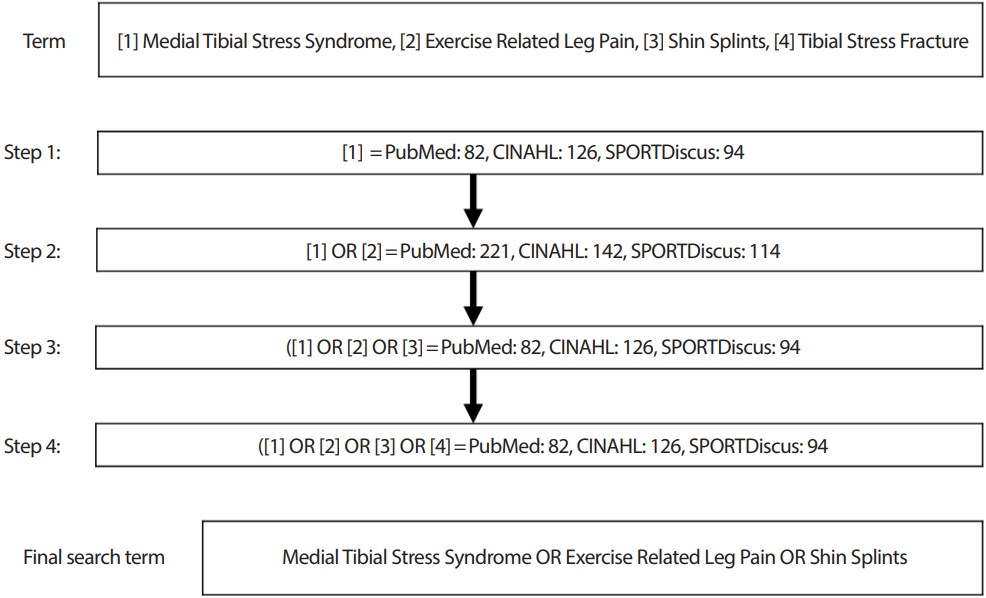
In order to include all potential studies, we used broad terms to search relevant studies. The broad terms, used for this review are different classifications of the overuse leg injuries. All relevant studies were searched through PubMed, CINAHL plus, and SPORTDiscus. The search was limited to human subjects and articles published in the English language between 1960 and 2018 using the search key words medial tibial stress syndrome; exercise related leg pain; shin splints; tibial stress fracture; combination of all the above terms. In order to identify and include other potential studies, all retrieved studies were cross-referenced as a final step for study selection. Fig. 1 illustrates the steps of search terms.
2. Study selection
A reviewer (HJ) performed the review process on all retrieved studies. Each individual study was identified and selected based on the criteria. The criteria for study inclusion were used as follows:
1) Studies had to focus on medial tibial stress syndrome/exercise related leg pain/shin splints/tibial stress fracture;
2) Studies had to evaluate kinematic variables related to rearfoot angle and/or tibial rotation;
3) Studies had to include the necessary statistical values
However, meta-analysis and review papers were excluded through our search procedure. Also, oral presentations and free communication were excluded. A reviewer did not perform contact with the authors for this paper.
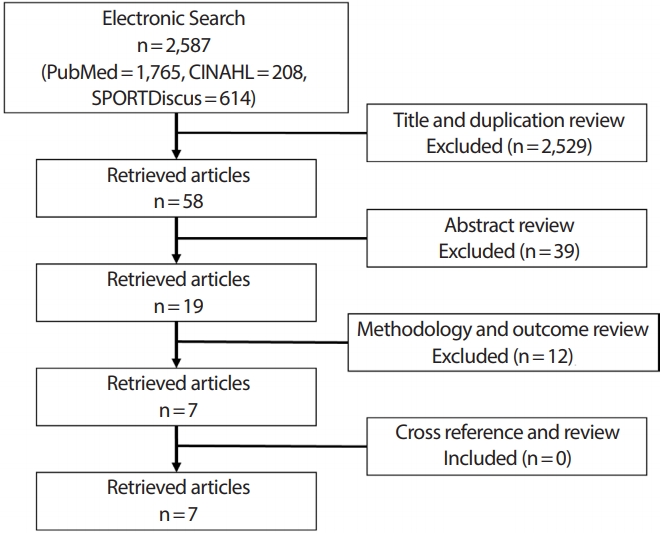
In addition, cross reference was performed on all selected studies. A total of seven studies were eligible for inclusion [5-9,11,12]. These studies were rated using the Physiotherapy Evidence Database (PEDro) which is an objective method with 10-point scale to determine the quality of methodology in each study. The details of the literature search and study selection were shown in Fig. 2.
3. Data extraction and analysis
Table 1 shows details of the allocation and blinding in all seven studies. We extracted mean and standard deviation of the rearfoot and tibia kinematic variables from both injured and control groups in each retrieved study to calculate Cohen’s d effect size (d=X ¯ 1 - X ¯ 2 S
RESULTS
A total of 7 studies were identified and selected in this review. The databases (PubMed, CINAHL plus, and SPORTDiscus) provided a total of 2,587 articles with duplication across three databases. 2,529 of those articles were excluded because those did not meet the criteria clearly through the title and abstract review.
After the review process, specific information was extracted from each selected study on: (1) type of study design; (2) inclusion and exclusion criteria; (3) outcome measure. Only two studies were conducted with prospective cohort study design while five studies used cross-sectional study design. None of selected studies were concealed the allocation and blinded as summarized in Table 1. Table 2 provides a brief summary of the specific inclusion and exclusion criteria, and the methodology for the individual studies in this review. Also, the specific kinematic variables related to rearfoot eversion and tibial internal rotation were reported in Table 2. To assess the quality of selected studies, Physiotherapy Evidence Data-base (PEDro) score of each individual study were reported in Table 2. A mean of PEDro score is 4.3 out of 10-point scale.
A total of 1,008 individuals were participated in all selected studies. The main inclusion criteria of subjects is adults between 18 and 45 years old. Two studies [11,12] included collegiate healthy population because the study design was the prospective-cohort design while the other studies [5-9] involved runners for cross-sectional design. Also, type of outcome variables was reported in Table 2 as described in section 2.3. In all studies, the outcome variables were measured between overuse leg injury group and no injury group.
A total of five studies examined rearfoot eversion between overuse injury and control group (Table 3, Fig. 3). The effect size for maximum rearfoot eversion from five studies ranged from -0.34 to 0.67 (All ES and 95% CI are reported in Fig. 3). Only three of five studies [9,11,12] explain that maximum rearfoot eversion during gait is significantly associated with MTSS, while two studies shows no significant difference in rearfoot eversion between overuse injury and control group. According to Cohen’s d index, all studies [9,11,12] showed medium effect with 0.64, 0.67, and 0.37, respectively (0.2 ≤d< 0.8).
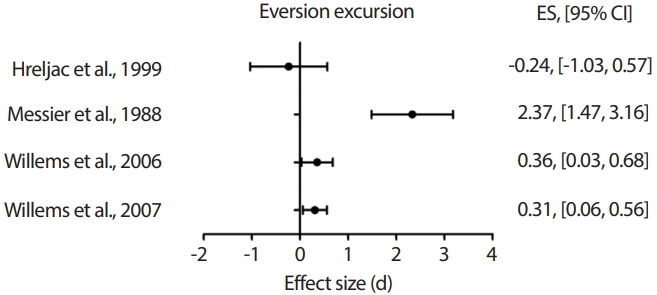
A total of four studies examined rearfoot eversion excursion during gait between overuse injury and control group (Table 4, Fig. 4). The effect size for eversion excursion from 4 studies ranged from -0.24 to 2.37 (All ES and 95% CI are reported in Fig. 4). Only one of these studies found no significant association with MTSS as a risk factor, while three studies [7,11,12] explain that rearfoot eversion excursion during gait is significantly associated with MTSS as highlighted on ES and 95% CI. Both studies by Willems et al. [11,12] showed medium effect with 0.31 and 0.36, respectively (0.2 ≤d< 0.8), while Messier et al., has ES of 2.37 represents a large effect (d≥ 0.8).
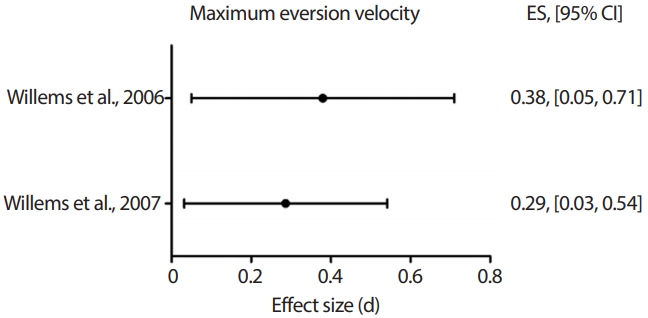
There were only two studies reported maximum eversion velocity with effect size 0.29 (95% CI: 0.03, 0.54) and 0.38 (95% CI: 0.05, 0.71) from all of 2 studies show statistically significance (Table 5, Fig. 5). Both ES of Willems et al. [11,12] represent medium effect based on Cohen’s index (0.2 ≤d< 0.8).
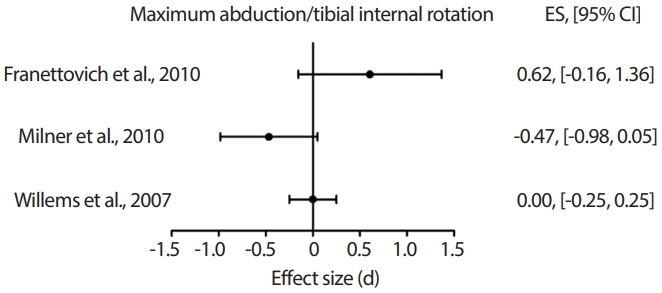
Three studies examined foot abduction/tibia internal rotation between overuse injury and control group (Table 6, Fig. 6). In this figure, none of 3 studies statistically significant with the effect sizes were ranged from 0.00 to 0.62 (All ES and 95% CI are reported in Fig. 6).
Three studies examined foot abduction excursion (Table 7, Fig. 7). The effect size for foot abduction excursion from 3 studies ranged from -0.04 to 0.35 but two of 3 studies [11,12] statistically significant with ES of 0.35 (95% CI: 0.02, 0.68) and 0.31 (95% CI: 0.06, 0.56), respectively, while one study shows no association as a risk factor of MTSS (All ES and 95% CI are reported in Fig. 7). Two studies by Willems et al. [11,12] represent medium effect with 0.35 and 0.31, respectively (0.2 ≤d< 0.8).
There were only two studies reported maximum foot abduction velocity and both studies [11,12] statistically significant with ES of 0.23 (95% CI: -0.02, 0.48) and 0.61 (95% CI: 0.28, 0.94), respectively (Table 8, Fig. 8). The ES of 0.61 and 0.23 from Willems et al. [11,12] represent medium effect (0.2 ≤d< 0.8, Table 8, Fig. 8).
DISCUSSION
The finding from this review paper confirmed that rearfoot and tibial motion are associated with MTSS during gait. Therefore, we accept the hypothesis; individuals with overuse injuries might have a more subtalar joint motion in the frontal (rearfoot motion) and transverse planes (tibial motion) based on the deviation of subtalar joint.
With the rearfoot kinematic variables from the literature, we found that most selected studies result in consistent greater rearfoot kinematic values in overuse leg injuries than healthy leg. However, one of the selected studies had a bias in the result because the rearfoot motion in healthy group is larger than MTSS group [6]. Most studies found that rearfoot motion in individuals with MTSS is greater than healthy individuals [7-9,11,12]. Therefore, the rearfoot eversion from the study by Hreljac et al. is located on opposite side to the other studies in Fig. 3 and 4. Based on these findings, we are able to strongly suggest that future research to develop a clinical prevention/treatment for restricting rearfoot motion is warranted.
On the other hand, we found that controversial results with the tibial kinematic variables from the same literature. Maximum foot abduction/ tibial internal rotation is not associated with overuse leg injuries during gait. Even though two studies [11,12] showed no significance in maximum foot abduction, they showed that foot abduction excursion and foot abduction velocity are associated with overuse leg injuries during gait. Only study by Franettovich et al. [5] showed consistent negative results in both maximum foot abduction and foot abduction excursion. We were not able to make recommendations on the tibial motion due to the insufficient evidence but we suggest that more future researches need to be conducted to justify a clinical prevention/treatment guideline.
This review paper used the PEDro score, represents the quality of selected studies. The mean of PEDro scores is 4.3 out of 10, is not a high quality. As allocation conceal and blinding of selected studies was reported in table 1, no study concealed allocation and blind the examiner. Because of the nature of injury pathology and methodology in selected studies, it is hard to perform a randomized control trial (RCT) study design. No RCT designed studies in literature result in low PEDro scores. Another limitation was sample size of individual selected study. There was only two studies reported power analysis for sample size. This could affect on the power of individual study.
The strength of recommendation (SORT) level is graded a 2A. Based on this level of evidence grade, this review paper suggests that restricting rearfoot motion (eversion) can prevent and treat overuse leg injuries. Restricting tibial motion (internal rotation) may affect on prevention and treatment for overuse leg injuries but it seems the effectiveness of restriction on tibial motion is less than rearfoot motion.
CONCLUSION
This review paper confirms that the kinematic characteristics of MTSS during gait. The rearfoot motion (eversion) associates with overuse leg injuries more than tibial motion (internal rotation). Based on this finding, the clinicians can consider rearfoot motion (eversion) to develop prevention and treatment program for overuse leg injuries including exercise-related leg pain, MTSS, shin splints, and/or tibial stress fracture. In addition, it is recommended that researchers need to perform RCT design to increase quality of evidence for future researches.